Here’s a 9 minute video demonstrating my easy technique for inserting a chest tube. I’ve included some helpful tips and tricks to make this a quick and easy procedure.

Here’s a 9 minute video demonstrating my easy technique for inserting a chest tube. I’ve included some helpful tips and tricks to make this a quick and easy procedure.
This short (10 minute) video demonstrated the technique for inserting small chest tubes, also known as “pigtail catheters.” It features Jessie Nelson MD from the Regions Hospital Department of Emergency Medicine. It was first shown at the third annual Trauma Education: The Next Education conference in September 2015, for which she was a course director.
Please feel free to leave any comments or ask any questions that you may have.

Related posts:
How To: Insert a regular chest tube for trauma
Pigtail catheters vs regular chest tubes
Tips for regular chest tubes
There’s lots of info out there on how to put a chest tube in. But what about on taking it out? There are a few nuances that you should be aware of so you can do this as quickly and complication-free as possible.
Have a look at this 5 minute video and let me know what you think. Please leave your comments on YouTube.

Traditionally, hemothorax and pneumothorax in trauma has been treated with chest tubes. I’ve previously written about some of the debate regarding using smaller tubes or catheters. A paper that will be presented at the EAST meeting in January looked at pain and failure rates using 14Fr pigtail catheters vs 28Fr chest tubes.
This was a relatively small, prospective study, and only 40 of 74 eligible patients were actually enrolled over 20 months at a Level I trauma center in the US. Pain was measured using a standard Visual Analog Scale, as was complication and failure rate, tube duration and hospital stay.
The following interesting findings were noted:
Bottom line: There may be some benefit in terms of tube site pain when using a smaller catheter instead of a chest tube. But remember, this is a very small study, so be prepared for different results if you try it for your own trauma program. If you do choose to use a smaller tube or catheter, remember to do so only in patients with a pure pneumothorax. Clotted blood from a hemothorax will not be completely evacuated.
Related posts:
Reference: A prospective randomized study of 14-French pigtail catheters vs 28F chest tubes in patients with traumatic pneumothorax: impact on tube-site pain and failure rate. EAST Annual Surgical Assembly, Oral paper 12, 2013.
I showed you this x-ray the other day, and asked what the problem was.
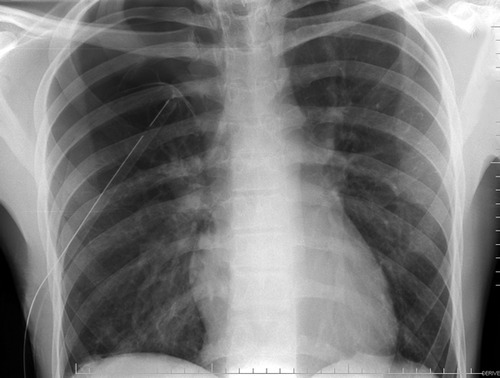
If you look carefully, you can see the lung outline in the middle of the right side of the chest. Big-time pneumothorax despite what looks like a perfectly placed tube. There are several possible explanations, and many of you sent me your guesses:
In this case the correct answer is the last one. This is one time when I would actually recommend a lateral chest x-ray. Have a look at the result. You can clearly see the tube snaking around into the soft tissues of the back.
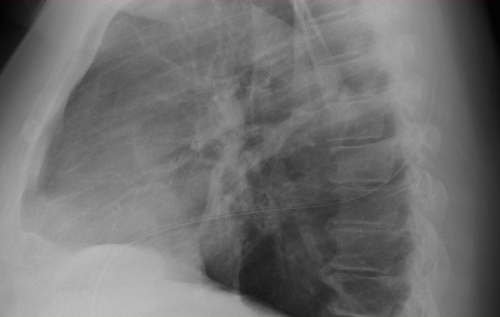
Bottom line: Remember that a perfect x-ray doesn’t necessarily mean a perfect tube. Go through the various possibilities quickly, and make it work.
Related posts: