I love stuff about chest tubes. There are so many opinions and so little data to back them up. And now here’s another EAST 2019 Annual Assembly paper from the University of Arizona at Tucson on chest tubes! The traditional dogma, and something that I’ve promoted for some time, is that the only size chest tube that should be used for hemothorax is big (36 Fr) or bigger (40 Fr). There have been a few abstracts and published papers over the past 7 years that are trying to change this assumption. Will they be successful?
The first work on this was a paper published in 2012 by this same group in Tucson. It was a prospective study that included 36 patients with pigtails and 191 with 32 Fr – 40 Fr chest tubes over 30 months. Average initial drain output was the same, and there were no differences in tube in time, complications, or failure rate.
A related abstract was then presented by this group at the 2013 EAST Annual Assembly, but it doesn’t look like this one got published. It was a small, prospective study that enrolled 40 of 72 eligible patients over 20 months and compared pigtail catheters vs 28 Fr chest tubes. They found that chest wall and tube site pain was less with a pigtail, and that failure and complication rates, tube in time, and hospital stay were the same.
And then in 2017 more related work was presented at EAST from the group, and was later published in the World Journal of Surgery. This study was the culmination of 7 years of experience, and included nearly 500 subjects. Once again, initial drainage output was the same, as were complications and failure rate. The authors concluded that a multi-center trial was need to provide additional support.
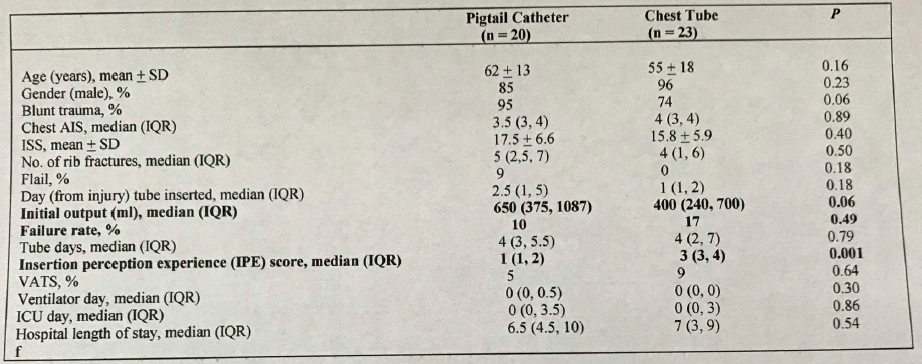
And that brings us up to EAST 2019. Now the authors are presenting a single-center study comparing 14 Fr pigtail vs 28-36 Fr chest tubes for hemothorax and pneumthorax. What’s different about this one? For the first time, the subjects were randomized between pigtail and chest tube in an effort to eliminate selection bias.
Here are the factoids:
- A total of 43 patients were enrolled, but the number excluded was not given
- Although baseline characteristics of the two groups were identical, several differences approached clinical significance: percent blunt trauma, flail chest, insertion day, and initial chest tube output
- The authors concluded that there were no differences in initial chest tube output, failure rate, tube days, and lengths of stay. However, perceived pain was less.
- They again noted that a multi-center trial should be performed to confirm these results
Here are some questions for the authors and presenter to consider in advance to help them prepare for audience questions:
- What’s new and different with this study? The University of Arizona – Tucson has been studying pigtails since 2009. Tell us about the progression of this work and how the current study fits in.
- How many patients were excluded? This is very important, especially if this number is high. What were the exclusion criteria exactly?
- What did your power analysis show? The overall enrollment numbers are low, which may throw your statistics into doubt. This is especially true since your primary outcome showed that pigtail and chest tube outputs were the same but with a p=0.06! More patients may have helped show the desired difference.
- Were the pigtail and chest tube groups really “similar?” There were more penetrating injuries in the chest tube group. Could this have an impact on clotted vs non-clotted blood in the chest and the ability of a pigtail to drain it? And the median pigtail insertion date was 1.5 days later than for chest tubes, which is clinically significant. Could this allow time for defibrination of the hemothorax, resulting in better drainage?
- And what’s next? Will I see you again at EAST 2020 or 2021 with a larger prospective study? Or a multi-center one?
I’m looking forward to hearing this one in person!
References:
- A single center prospective randomized study comparing the effectiveness of 14 French percutaneous catheters (pigtail) versus 28-36 French chest tube in the management of traumatic hemothorax/hemopneumothorax. EAST 2019 Paper #13.
- EAST abstract presentation 2013.
- EAST abstract presentation 2017.

