In my last post, I described a long-standing whole blood transfusion program that was implemented by Royal Caribbean Cruise Lines (RCCL)about 10 years ago. Today, I’ll dig into the specifics of their protocol and review their results.
Here is an image of the protocol. You can click it to download a full-size pdf copy.
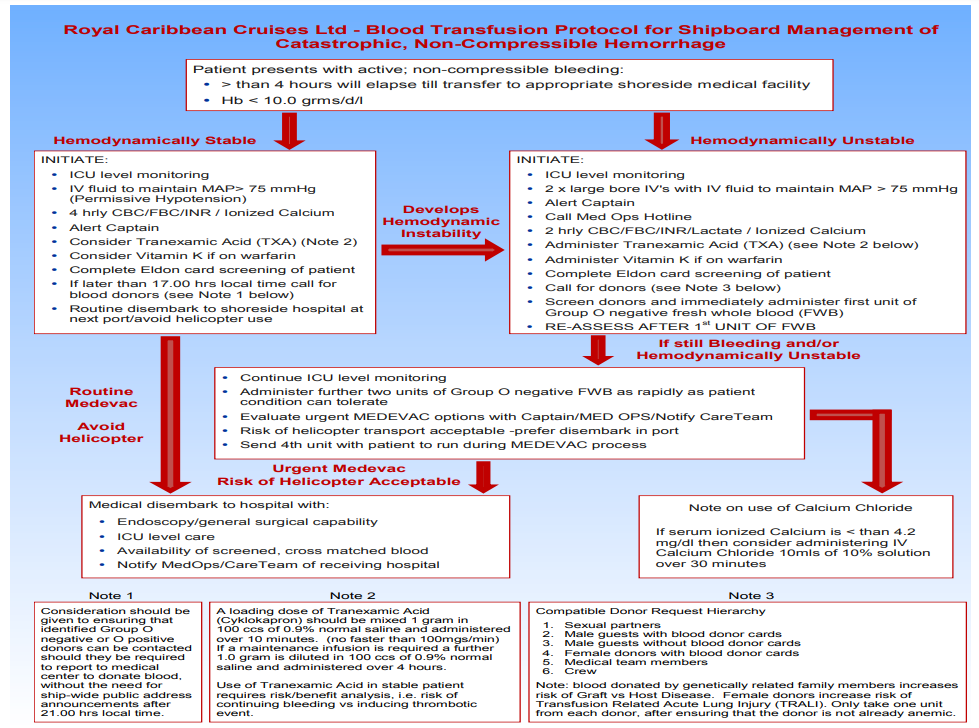
Here are the key points in the protocol:
- It is only implemented if it will take more than 4 hours to get the patient ashore for more advanced care
- If the patient is hemodynamically stable, permissive hypotension to MAP 75 is encouraged and TXA infusion / Vitamin K administration are considered when appropriate. The patient disembarks at the next port of call with advanced hospital capabilities.
- If hemodynamically unstable, two large bore IVs are maintained, TXA and Vitamin K are given when appropriate, and whole blood collection and administration are initiated. Helicopter / coast guard transport is deemed acceptable to closest advanced hospital.
And here are the guidelines for donor selection:
- The donor hierarchy is:
- sexual partner of the patient
- male passenger with blood donor card
- male passenger without blood donor card
- female passenger with blood donor card (beware of TRALI)
- medical staff members
- crew
- Only one unit is taken from each donor, and they must not be anemic
Here are the factoids describing RCCL’s seven year experience with the program:
- 73 patients received transfusions, including 67 passengers and 6 crew
- Mean hemoglobin on presentation was 6
- A total of 1-6 units were given
- Six patients ultimately died; no details were given
- There were no ABO seroconversions, and only two adverse reactions occurred, both allergic
- The majority of the medical staff felt that this was a valuable program
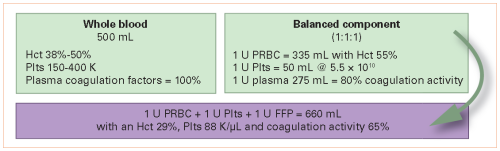
Bottom line: This is the first whole blood transfusion program I have seen outside of hospitals and the military. Royal Caribbean has incorporated lessons learned from both in developing their protocol. It includes all the principles of balanced resuscitation, including limiting crystalloids, permissive hyportension, and 1:1:1 transfusion ratios. There are many other opportunities to implement similar protocols in areas where medical capabilities are austere, and this protocol should be used as a model to develop them.