I’ve written many posts in the past about the arguments surrounding chest tube size: large bore vs. small bore (pigtail). For the longest time, only a few decent papers were looking into this debate, and subject numbers were small. The best the papers could say was that “small-bore chest tubes are not inferior to large-bore tubes.” Not that this is not the same as saying, “small-bore tubes are better than large-bore tubes.”
But finally, after more than ten years, there has been enough written on the topic that a pass at a systematic review and meta-analysis has been attempted. The University of Miami Ryder Trauma Center group performed a comprehensive review of the topic, spanning literature published through 2022.
Here are the factoids:
- A total of 2008 articles were identified, but after careful screening, only 11 articles met predetermined parameters for inclusion
- There were 3 randomized, controlled studies, 3 prospective cohort studies, and 5 retrospective cohort studies
- Two pairs of studies had overlapping patients, so only patients in the more recent study of each was included
- The authors used CASP scoring to judge the quality and likelihood of bias. Nearly all studies included were of high quality.
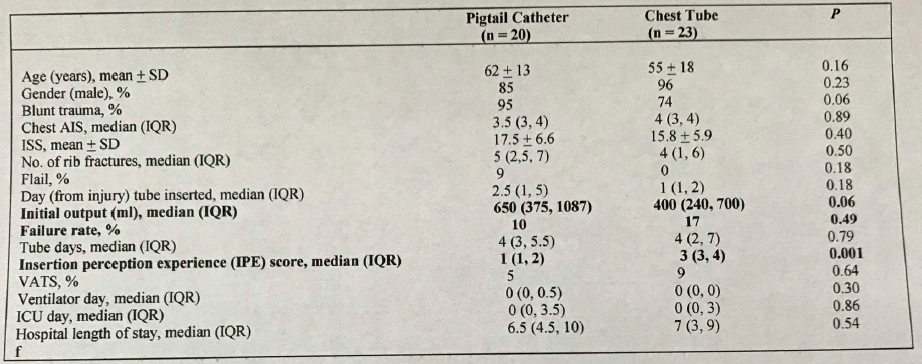
And here are the interesting findings:
- There was no significant difference in failure rates between small and large tubes (18% vs. 22% )
- There were no differences in complication rates (12% vs. 13% )
- There was a significantly higher amount of initial drainage with the small tubes (750 cc vs 400 cc) (??)
- Although the overall number of complications was the same, there were significantly more insertion complications in the small-bore group (4.4 vs 2.2). These included intra-hepatic placement, malpositioned tubes, kinked tubes, and dislodgement.
- Only one study used a validated pain score to measure insertion pain, and there was no difference between the tube sizes
- Tube days averaged 1.5 days less in the small-bore group, which was significant. However, this did not impact ICU or hospital length of stay.
Bottom line: There are still significant limitations in this study due to the small number of randomized controlled trials that are yet available. I also worry that there is some selection bias in many of the studies that would cause large-bore tubes to be inserted preferentially into patients with more severe chest trauma, larger hemothorax, or more emergent need for the tube. However, if there were major, major differences, they would probably be starting to rear their heads by now.
The authors of this paper concluded that “small bore tube thoracostomy may be as effective as large bore thoracostomy for the management of patients with hemothorax.” They correctly suggest that guided studies examining which patients are more suited for a specific sized tube. I totally agree.
For now, I still don’t think there is a definitive answer. I recommend that the bedside trauma professional use their judgment regarding patient condition, the magnitude of the chest trauma, and the urgency of the procedure to select a size. They must also consider their expertise with the tube selected to maximize effectiveness and minimize complications.
I’m sure there will be even more to write on this topic. It doesn’t seem to want to die.
Reference: Small versus large-bore thoracostomy for traumatic hemothorax: A systematic review and meta-analysis. Journal of Trauma and Acute Care Surgery 97(4):p 631-638, October 2024. | DOI: 10.1097/TA.0000000000004412