Trauma resources (centers and helicopter services) are not geographically evenly distributed across the US. The East and West coasts are saturated with resources, maybe overly so. At the other extreme, some northern states (Alaska and the north central US) have very few trauma resources, and injured patients may have to travel several hundreds of miles to get definitive trauma care.
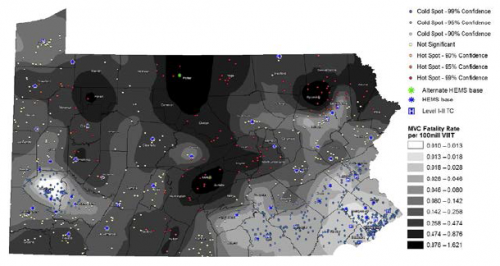
The group at the University of Pittsburgh looked at trauma resource distribution across the state of Pennsylvania, and matched that with geographical data from fatal car crashes over a two year period. They used some special statistical tools to analyze this type of data, and reported their findings in a format that will be unfamiliar to many: fatalities per 100 million vehicle miles traveled (VMT).
Here are the factoids:
- 863 fatal crashes occurred during the study period, killing 884 people
- The median fatality rate for the state was .187 per 100 million VMT
- Fatality hotspots became very apparent in areas farther from trauma system resources (TSR) (see map below, dark areas are bad)
- The fatality rate increased significantly by 0.01 per 100 million VMT for each mile farther away from any TSR.
- If just 2 helicopters had been relocated from trauma centers to high fatality regions, the overall fatality rate could have been reduced by 12%, in theory
Bottom line: This novel way of looking at injury data confirms what we all knew or suspected: injuries occurring farther away from trauma resources may lead to higher mortality and disability. And knowledge is power. If we can see it, we can do something about it. This type of analysis should be done on regional, state, and national levels to help us better serve our patients.
Questions and comments for the authors/presenters:
- Be able to describe your statistics simply
- How did you deal with data from the border areas of the state? Did you include trauma resources from adjacent states in your analysis?
- You mention “county-level” factors in adjusting mortality rates for distance. What were these?
- This is a novel way of approaching system planning. Nice job!
Click here to go the the EAST 2017 page to see comments on other abstracts.
Related post:
Reference: Distance matters: effect of geographic trauma system resource organization on fatal motor vehicle collisions. Paper #3, EAST 2017.