The standard of care in most high level trauma centers is to involve neurosurgeons in the care of patients with significant traumatic brain injury (TBI). However, not all hospitals that take care of trauma patients have immediate availability of this resource. An interesting paper looked at management of these patients by acute care surgeons.
The authors retrospectively reviewed all their patients who had a TBI and positive head CT managed with or without neurosurgery consultation over a two year period. They matched the patients with and without neurosurgical consultation for age, GCS, AIS-Head and presence of skull fracture and intracranial hemorrhage (parenchymal, epidural, subdural, subarachnoid). Neurosurgeons were available to the no-consult group if things went awry.
A total of 180 patients with and 90 patients without neurosurgical involvement were reviewed. Here are the interesting findings:
- Hospital admission rate was identical for both groups (88%)
- ICU admission was significantly higher if neurosurgeons were involved (20% vs 44%)
- Repeat head CT was ordered more than 3 times as often by neurosurgeons (20% vs 86%)
- Post-discharge head CT was ordered more often by neurosurgeons, but was not significantly higher (5% vs 12%)
- There were no neurosurgical interventions, in-hospital mortalities, or readmissions within 30 days in either group
Based on this experience, the hospital adopted a set of guidelines for helping determine if neurosurgery should be consulted.
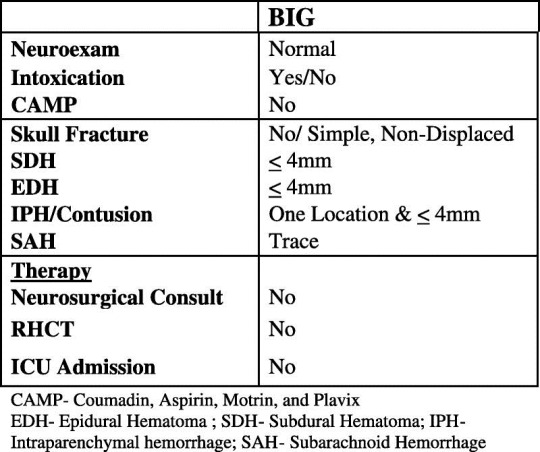
Bottom line: This work raises an interesting question: can general surgeons safely manage select patients with intracranial injury? The answer is probably yes. The majority of patients with mild to moderate TBI with small intracranial bleeds do well despite everything we throw at them. And it appears that surgeons use fewer resources managing them than neurosurgeons do. The keys to being able to use this type of system are to identify at-risk patients who really do need a neurosurgeon early, and having a quick way to get the neurosurgeon involved (by consultation or hospital transfer). Looking at the brain injury guidelines above, I am a little nervous about managing an epidural or contusion without one additional head CT. But this is certainly food for thought. As neurosurgery involvement in acute trauma declines, this concept will become more and more pertinent.
Related posts:
Reference: The acute care surgery model: managing traumatic brain injury without an inpatient neurosurgical consultation. J Trauma 75(1):102-105, 2013.
