I reviewed this abstract a few months ago, and now I’ve had the opportunity to hear it and see the data. Here’s an update on whether this is worthwhile..
This was a relatively small, prospective study, and only 40 of 74 eligible patients were actually enrolled over 20 months at a Level I trauma center in the US. Pain was measured using a standard Visual Analog Scale, as was complication and failure rate, tube duration and hospital stay.
The following interesting findings were noted:
- Chest wall pain was similar. This is expected because the underlying cause of the pneumothorax, most likely rib fractures, is unchanged.
- Tube site pain was significantly less with the pigtail
- The failure rate was the same (5-10%)
- Complication rate was also the same (10%)
- Time that the tube was in, and hospital stay was the same
There were a few questions regarding blinding of the pain scale raters, but other than the small sample size, the study was nicely done.
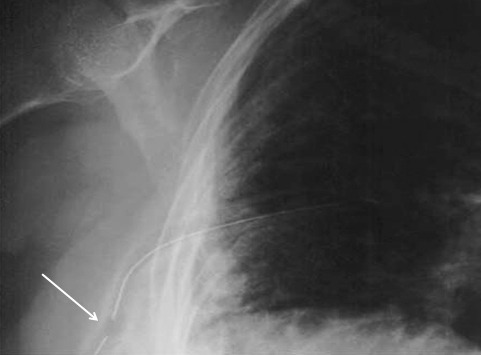
Bottom line: There may be some benefit in terms of tube site pain when using a smaller catheter instead of a chest tube. But remember, this is a very small study, so be prepared for different results if you try it for your own trauma program. If you do choose to use a smaller tube or catheter, remember to do so only in patients with a pure pneumothorax. Clotted blood from a hemothorax will not be completely evacuated.
Related posts:
Reference: A prospective randomized study of 14-French pigtail catheters vs 28F chest tubes in patients with traumatic pneumothorax: impact on tube-site pain and failure rate. EAST Annual Surgical Assembly, Oral paper 12, Jan 17, 2013.