Kids are frequent flyers when it comes to abdominal injury, with about 15% of their injuries involving this anatomic area. Solid organ injuries, mainly the liver and spleen, are the most prevalent ones. The American Pediatric Surgical Association (APSA) published a practice guideline way back in 2000 that outlined a consistent way to care for children with solid organ injuries.
Unfortunately, they were very conservative, recommending days of bedrest, extended NPO status, very frequent blood draws, and a lengthy hospital stay. Many hospitals, including mine, developed less conservative management routines, noting that children nearly always tolerate liver and spleen injury better than adults.
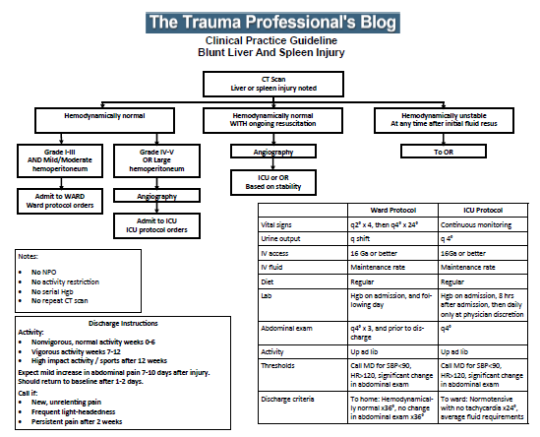
The trauma group at Vanderbilt modified the APSA guidelines and, more recently, made additional changes based on a new algorithm released by the organization. This new guideline moved away from organ injury grade-based factors and embraced hemodynamic status as the overall guide to care. The Vanderbilt group performed a retrospective study comparing hospital and ICU length of stay, patient costs, readmission, and death rates using the two guidelines.
Under the old protocol, grade I-III injuries were admitted to a floor bed and higher grades to an ICU at the discretion of the surgeon. The minimum hospital stay was, at minimum, the organ injury grade. Children were kept NPO overnight and placed on bed rest for nearly one day per injury grade.
With the new protocol, children were admitted to the floor if their vital signs normalized after volume resuscitation. Hematocrit was obtained on admission and possibly again after 6 hours, then only repeated if < 21 or a change in vitals was noted. There were no diet or activity restrictions. Children with abnormal vital signs after volume were admitted to the ICU and kept on bed rest until they normalized. Labs were drawn regularly. Length of stay was based on meeting pain control, diet, and activity goals.
Here are the factoids:
- There were 176 children (age < 18) enrolled in the old protocol during a four-year period and 170 in the new protocol over 3.5 years
- Both groups were similar demographically and in injury grade and ISS
- ICU length of stay was “significantly” shorter under the new protocol (.54 vs .78 days)
- Hospital length of stay was also “significantly” shorter (2.9 vs 3.5 days)
- Inflation-adjusted costs were slightly higher under the new protocol ($68,042 vs $65,437) even though the authors claim the opposite in the abstract once injury grade and ISS are factored in
- Survival was the same at 99.4%
- Readmission rates were significantly higher under the new protocol (7.1% vs 2.3%)
The authors’ conclusions parroted these results and recommended larger studies to detail any cost advantage and identify the cause for the difference in readmission rates.
Bottom line: This study leaves a lot to be desired. The authors’ definition of “pediatric” is age < 18. As we all know, there is a big difference in “kids” who are pre- vs post-puberty. The good news is that the mean and median ages are about 11 in the study, so there should be fewer older “kids” to cause interference.
The authors reported hazard ratios for the lengths of stay, which were statistically significantly different. However, their clinical significance is in doubt. A difference of 6 ICU hours? Or two-thirds of a hospital day? I’m not impressed.
Cost differences are basically a wash, and a deep read of the paper shows that many kids did not have an isolated solid organ injury. Non-abdominal injuries could have an Abbreviated Injury Scale score of up to 3. It is easy to imagine that these could impact both length of stay and cost.
Finally, the readmission rates include many problems related to non-abdominal injuries, including the thorax, soft tissues, and even an epidural hematoma. After excluding these non-abdominal complications, the numbers for both protocols are so low it’s hard to believe that a good significance test can be performed.
The authors’ conclusions are correct: more work needs to be done. This paper doesn’t really teach us much since all the conclusions are extremely weak. A much better, prospective, multicenter trial should be performed. Unfortunately, getting buy-in from multiple centers/surgeons to use the same protocol in children is hard.
But with all that being said, there is no reason you can’t adopt something similar to the new protocol at your center. My own experience has shown that a more aggressive guideline gets kids home sooner and healthier and that there is no difference in readmission rates. I just need a bunch of other surgeons to duplicate these results and write them up!
Reference: A Protocol Driven Approach to Reduce Lengths of Stay for Pediatric Blunt Liver and Spleen Injury Patients. Journal of Trauma and Acute Care Surgery ():10.1097/TA.0000000000004259, January 26, 2024. | DOI: 10.1097/TA.0000000000004259