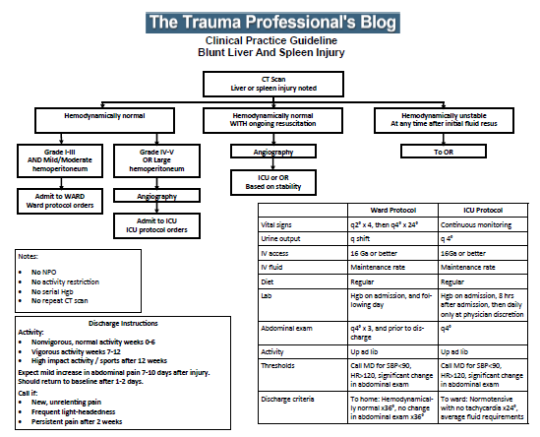
Over the past several days, I’ve been writing about updates to our solid organ injury protocol. It eliminates orders for bed rest and NPO diet status afterwards. After looking at our experience over the years, the number of early failures is practically zero. So how many days do you need to keep a patient in bed to make sure they have an empty stomach when they need to be whisked away to the OR. And does walking around really make your injured spleen fall apart?
The answers are none and no. So we’ve updated our protocol at Regions Hospital to reflect this. Feel free to download and modify to your heart’s content. If you want a copy of the Microsoft Publisher file, just email me!
Over the years, I’ve written about solid organ injury management many times. Here is a summary of some practical pointers and tips, some old and some new. They are as evidence-based as I can get them. This kind of stuff is not always in the doctor and nursing books.
Ward and ICU branches are order sets at my hospital, not necessarily admitting locations. If you have a special unit or step-down area that can provide ICU-level monitoring, use it for the ICU order set.
Strongly consider interventional radiology (IR) and angiography in all adult patients with contrast extravasation (children generally do not qualify unless they show signs/sx of ongoing volume loss). Consider also in high grade injuries, because they may have active bleeding that isn’t quite brisk enough to see on CT.
Serial hemoglobin measurements are not part of the protocol. They are only used to help decide if transfusion might be needed. Vital signs will always signal failure before the hemoglobin does.
Nearly all patients may be up and eating immediately, or certainly by the next morning. No need for protracted NPO status or bed rest. Really no need for it at all!
Failure really falls into 2 types: hard and soft. Hard failure is a single episode of definitive hypotension (usually 80s or less) or development of peritoneal signs, and requires an emergency trip to the OR. Soft failure is transient or modest hypotension that responds rapidly to a fluid bolus. If IR has not already been used, a quick trip there may obviate the need for operation. However, another one of these bouts makes it a hard fail. Time for OR.
Hard failure can only be treated with blood, some crystalloid, and a knife. Pressors, steroids, or other drugs can only be used if they come in liter bags and can be given at over 1000cc/hr. That means never.
In IR, give the radiologist 30 minutes to stop the bleeding. Don’t let them dawdle for hours. If the patient has a hard fail, abort and go to OR; do not let the radiologist persist.
After discharge, our usual orders are:
Normal activity (non-impact) for 6 weeks
All activity (except high impact) thereafter
High impact activity (tackle football, rugby, serious extreme sports) only after 12 weeks (no good data for this one)
No repeat CT scanning to judge healing
Warn patients of the good possibility of a transient increase in pain on days 7-10. This is common in many unless they’ve been embolized.
Patient to call if unrelenting increase in pain, or increasing orthostatic symptoms, fevers chills
Any trauma professional who has dealt with spleen injuries knows that the white blood cell (WBC) count rises afterwards. And unfortunately, this elevation can be confusing if the patient is at risk for developing inflammatory or infectious processes that might be monitored using the WBC count.
Is there any rhyme or reason to how high WBCs will rise after injury? What about after splenectomy or IR embolization? An abstract is being presented at the Clinical Congress of the American College of Surgeons next month that examines this phenomenon.
This retrospective study looked at a convenience sample of 75 patients, distributed between patients who had splenic injury that was either not treated, removed (splenectomy), or embolized. Data points were accumulated over 45 days.
Here are the factoids:
20 patients underwent splenectomy, 22 were embolized, and 33 were observed and not otherwise treated
Injury severity score was essentially identical in all groups (19)
Splenectomy caused the highest WBC counts at the 30 day mark (17.4K)
Embolized patients had mildly elevated WBC levels (13.1K) that were just above the normal range at 30 days
Observed patients had high normal WBC values (11.0K) after 30 days
Values in observed and embolized patients normalized to about 7K after 30 days; splenectomy patient WBC count remained mildly elevated at 14.1K.
The authors concluded that embolization does not result in permanent loss of splenic function (bad conclusion, rookie mistake!)
Bottom line: This study is interesting because it gives us a glimpse of the time course of leukocytosis in patients with injured spleens. If you need to follow the WBC for other reasons, if gives a little insight into what might be attributable to the spleen. Splenectomy generally results in a chronically elevated WBC count, which tends to vary in the mid-teens range. Embolization (in this study) transiently elevates the WBC count, but it then drops back to normal.
The big problem with this study (besides it being small) is that it fails to recognize that there are many different shades of embolization. Splenic artery? Superselective? Selective? I suspect that the WBC count in main splenic artery embolization may behave much like splenectomy in terms of leukocytosis. And the conclusion about splenic function being related to WBC count was pulled out of a hat. Don’t believe it.
Leukocytosis after Splenic Injury: A Comparison of Splenectomy, Embolization, and Observation. American College of Surgeons Scientific Forum Abstracts pg S164, 2015.
A set of guidelines for management of blunt solid organ injury in children developed by the American Pediatric Surgical Association was originally published in 1999. One of the elements of the guideline was to place the child on bedrest for a period of time after the injury. Arbitrarily, this period was defined as the injury grade plus one day. So for a grade 3 spleen injury, the child would have to stay in bed for 4 days (!).
Recent work looked at the impact of shortening this time interval. Over a 6 year period, all pediatric liver and spleen injuries from blunt trauma were identified and an abbreviated bedrest protocol was implemented. For low grade injuries (grade 1-2), children were kept in bed for 1 day, and for higher grade injuries this was extended to 2 days.
Here are the factoids:
249 patients were enrolled (about 40 per year) with an average age of 10. “Bedrest was applicable for 199 patients, 80%.” Huh? Does that mean that 50 patients were excluded due to surgeon preference?
The organ injured was about 50:50 for spleen vs liver. Twelve children injured both.
Mean injury grade was 2.7, which is fairly high
Mean bedrest was 1.6 days, and mean hospital stay was 2.5
Bedrest was the limiting factor for hospital stay in 62% of cases
There were no delayed complications of the injury
Bottom line: Come on! Most centers don’t keep adult patients at bedrest this long, and we learned about solid organ injury management from kids! Children almost never fail nonop management, so why treat them more restrictively than adults? And have you ever tried to keep a child at bedrest? Impossible! This study is too underpowered to give real statistically valid results, but it certainly paints a good picture of what works. We’ve been keeping both adults and children at bedrest only overnight, and our average length of stay for isolated solid organs is about 1.5 days. But really, who says that staying in bed for any period of time avoids complications? There are lots of other evil things that can happen!
Reference: Follow up of prospective validation of an abbreviated bedrest protocol in the management of blunt spleen and liver injury in children. J Ped Surg 48(12):2437-2441, 2013.
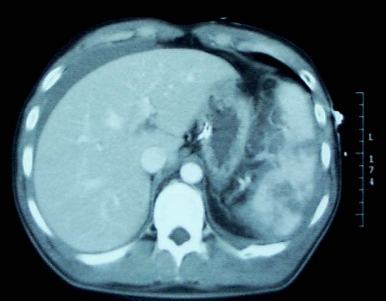
A contrast blush is occasionally seen on abdominal CT in patients with solid organ injury. This represents active arterial extravasation from the injured organ. In most institutions, this is grounds for call interventional radiology to evaluate and possibly embolize the problem. The image below shows a typical blush.
This thinking is fairly routine and supported by the literature in adults. However, it cannot be generalized to children!
Children have more elastic tissue in their spleen and tend to do better with nonoperative management than adults. The same holds true for contrast blushes. The vast majority of children will stop bleeding on their own, despite the appearance of a large blush. In fact, if children are taken to angiography, it is commonplace for no extravasation to be seen!
Angiography introduces the risk of local complications in the femoral artery as well as more proximal ones. That, coupled with the fact that embolization is rarely needed, should keep any prudent trauma surgeon from ordering the test. A recently released paper confirms these findings.
The only difficult questions is “when is a child no longer a child?” Is there an age cutoff at which the spleen starts acting like an adult and keeps on bleeding? Unfortunately, we don’t know. I recommend that you use the “eyeball test”, and reserve angiography for kids with contrast extravasation who look like adults (size and body habitus).