Here’s an interesting case for you to pick apart!
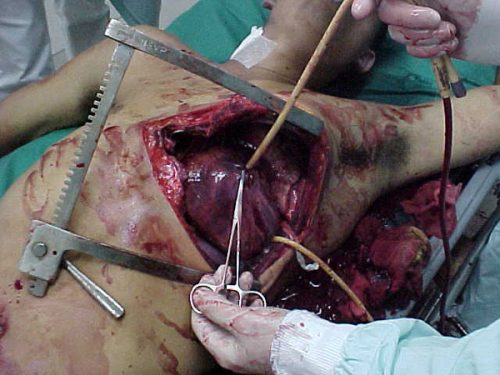
A 25 year old man is involved in some sort of violent, non-productive interpersonal relationship. He sustains a stab to the left chest, and is brought to your trauma center as a trauma team activation. During the FAST exam, a moderate effusion with visible clot is seen in the pericardium.
Appropriately, you run to the OR and prepare for a left thoracotomy. You perform a pledgeted repair of the ventricle and close. The patient does well and is discharged home five days later. He returns to your clinic the following week and is doing well. You remove the staples.
One week later, he returns to your emergency department complaining of significant chest pain. He describes it as deep, behind his sternum, and it seems to be exacerbated by breathing.
Now what? What are you thinking about? What additional exam do you need. What labs?
Tweet or comment with your answers and suggestions. More on Monday!