The data we use as guidance for repeat head CT in elderly patients who sustain mild TBI while taking antithrombotic therapy remains limited. There is a slowly growing consensus that the need is limited, but there is still a very wide variation in practice patterns.
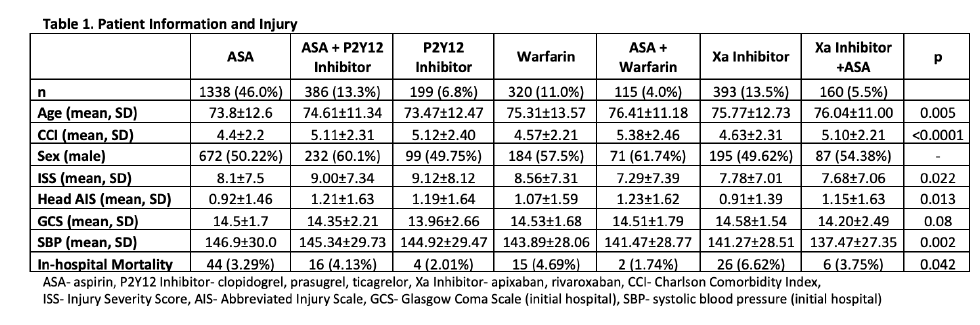
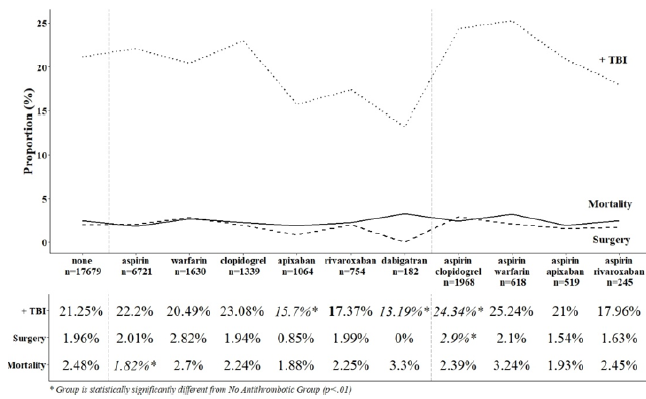
The group at HCA Healthcare Nashville collected data from 24 system hospitals on this very specific cohort of patients: elderly (age > 55), head trauma with GCS 14-15, an initial head CT, and no other injuries with AIS > 2. They divided these patients into two groups based on whether they were currently taking antithrombotic (AT) therapy. Rate of delayed intracranial hemorrhage (ICH), need for neurosurgical intervention, and mortality were compared.
Here are the factoids:
- About 3,000 patients were enrolled and only 10% had a repeat head CT
- Of those who were rescanned, 10% of patients on meds had a new ICH vs 6% in those not taking meds (not statistically significant)
- Extrapolating those numbers to all patients, the rate of delayed ICH would be 0.7% in patients not taking AT vs 1.0% for those who were (also not significant)
- Mortality attributable to a head bleed occurred in only one patient who was made comfort care
- There were no neurosurgical procedures performed in either group
The authors concluded that this specific subset of patients has a very low rate of delayed ICH, and that there are minimal clinical consequences in those that do. They do not support repeat head CT.
Bottom line: This abstract adds to the growing body of literature that shows little benefit to repeat head CT scan after a negative initial study, even if the patient is on blood thinners. Many previous studies involve only a single center and/or have smaller numbers. This one is larger because of the size of the HCA trauma system, and answers a simple set of questions on a limited subgroup of patients: elderly, mild TBI, with limited other injuries.
My back of the envelope power calculations show the authors may be a little short of the number of subjects to be able to show that the difference in the number of delayed ICH (0.7% vs 1.0%) is statistically significant. But the numbers are close enough and the p value so large (0.3) that they are probably right. This is completely offset by the absence of necessary neurosurgical interventions and the single attributable death.
Many trauma centers, including my own, have adopted a “no repeat scan” policy after a negative initial scan, even on thinners. In fact, unless the patient has some other injury that requires admission, they are discharged home with a responsible adult.
Here are my questions for the authors and presenter:
- Did you do any type of power analysis to determine if the large number of patients included was actually large enough?
- The term “antithrombotic therapy” is used broadly; which agents were considered in this category? Traditional warfarin therapy? Aspirin and other antiplatelet agents? DOACS?
- Have you changed your system guidelines to reflect your work?
This is important and practical work! I’m looking forward to hearing all the details.
Reference: ROUTINE REPEAT BRAIN CT SCANNING IS UNNECESSARY IN OLDER PATIENTS WITH GCS 14-15 AND A NORMAL INITIAL BRAIN CT SCAN REGARDLESS OF PREINJURY ANTITHROMBOTIC USE: A MULTICENTER STUDY OF 3033 PATIENTS. EAST 35th ASA, oral abstract #31.