Solid organ injuries are relatively common from both blunt and penetrating mechanism due to the fact that the liver is the largest organ in the torso. Management of minor injury is relatively straightforward, but more complex injuries quickly become complicated. Unlike the spleen, there is no option to just “drop it in the bucket.” And recovery from high-grade hepatic injuries is fraught with issues like bleeding and bile leaks. These patients may take weeks or months to fully recover.
A wide variety of operative techniques for controlling liver bleeding were developed in the 1900s. These became a little less relevant late in the century with the addition of angiography and embolization to our suite of management techniques. Remember, angioembolization does not replace operative management, which is mandatory in unstable patients. But it can certainly help control bleeding and may reduce the need to operate early.
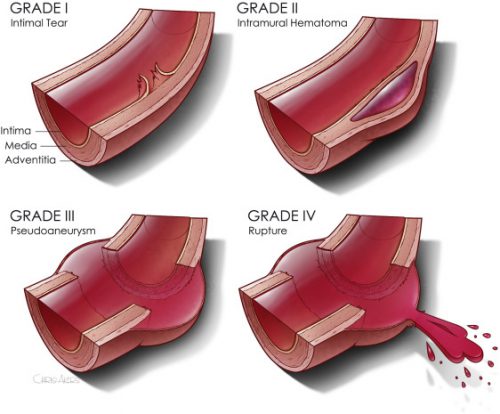
The group at Johns Hopkins hypothesized that angioembolization (AE) improves survival in patients with severe hepatic injuries. They collected data from 29 trauma centers in an AAST multicenter study. It focused on adult patients with Grade III-V injury from either blunt or penetrating mechanism. The data were sliced and diced by mechanism and type of management. There were three management possibilities: nonop management with or without AE, operative management with AE before or after, and operative management alone.
Here are the factoids:
- A total of 1,697 blunt and 733 penetrating liver injury patients were studied with similar median ISS
- As expected, higher ISS and blood transfusion > 6u was significantly associated with higher mortality
- In the blunt injured patients managed nonoperatively, there was no association between mortality and use of AE although the p value was 0.056
- Similarly, blunt trauma patients who underwent an operation and had AE either before or after had no difference in mortality (p value 0.09)
- There was a significant survival advantage if AE was added to nonoperative management
The authors concluded that angioembolization does not improve survival in most severe liver injury cases with the exception of high-grade penetrating injury.
Bottom line: This abstract focuses on survival advantage from the use of AE. However, I think most trauma professionals actually use it as an adjunct to make other management (operative or nonoperative) easier. So I’m not surprised that they didn’t find much positive to say except in the case of penetrating injuries.
I also worry that the p values for both groups of blunt patients (operative + AE, nonop + AE) were very close to significance. Any time a study provides a negative conclusion because significance was not reached, I want to be sure it had the statistical power to detect it in the first place. With p values of 0.09 and 0.056, could a few more patients in each group have achieved statistical significance?
I don’t see that this abstract could (or even should) change our practice in the use of AE. I suspect that it does have an impact on complications, and it may help us stay out of the abdomen in severe cases where opening it could result in uncontrollable bleeding.
Here are my questions and comments for the authors / presenter:
- Did you do a power analysis to determine if you could actually show a significant difference in the blunt patients? Although you had 1,697 total blunt patients, we do not know how many were in the operative vs nonop groups and the AE vs no AE subset of the nonop management group.
- Were there any differences in the ISS, age, or other demographics in the pre vs post or AE/no AE blunt subsets that might reveal some selection bias for patients undergoing in one subset vs the other? Since this is pooled data from many trauma centers, each surgeon determines if AE is used and when. It becomes very important to try to identify other factors that may explain your results.
- Do you recommend any changes in clinical care based on these results? What needs to be done to definitively answer the question?
This is interesting preliminary work, but I believe it needs additional refinement before we learn enough to change our current practice.
Reference: AAST MULTICENTER STUDY: DOES ANGIOEMBOLIZATION IMPROVE SURVIVAL FOR SEVERE HEPATIC INJURIES? AAST plenary paer #51, AAST 2022.