Hello sports fans! My trauma center(s) are undergoing our own Level I adult and pediatric verification visits today and tomorrow. I’ll be taking a break and getting back to you on Wednesday.
See you then!
Michael
![]()

Hello sports fans! My trauma center(s) are undergoing our own Level I adult and pediatric verification visits today and tomorrow. I’ll be taking a break and getting back to you on Wednesday.
See you then!
Michael
![]()
Many surgeons and surgical subspecialists are nervous about operating on people who are taking anticoagulants. This seems obvious when it involves patients on therapeutic anticoagulation. But it is much less clear when we are talking about lower prophylactic doses.
Spine surgeons are especially reluctant when they are operating around the spinal cord. Yet patients with spine injury are generally at the highest risk for developing venous thromboembolic (VTE) complications like deep venous thrombosis (DVT) or pulmonary embolism (PE). Is this concern warranted?
Surgeons at the Presley Trauma Center in Memphis examined this issue by performing a retrospective review of six years worth of patients who underwent spine stabilization surgery. They specifically looked at administration of any kind of preop prophylactic anticoagulant, and the most feared complications of bleeding complications and postop VTE.
Here are the factoids:
Bottom line: So what to make of this? It’s a relatively small, retrospective study, and there is no power analysis. Furthermore, this hospital does not perform routine DVT screening, so that component of VTE may be underestimated, rendering the conclusions invalid.
However, the information on bleeding complications is more interesting, since this is much more reliably diagnosed using an eyeball check under the dressing. So maybe we (meaning our neurosurgeons and orthopedic spine surgeons) need to worry less about preop prophylactic VTE drugs. But we still need better research about whether any of this actually makes a dent in VTE and mortality from PE. To be continued.
Reference: Early chemoprophylaxis is associated with decreased venous thromboembolism risk without concomitant increase in intraspinal hematoma expansion after traumatic spinal cord injury. J Trauma 83(6):1108-1113, 2017.
Deer hunting season is upon us again in Minnesota and Wisconsin, so it’s time to plan to do it safely. Although many people think that hunting injuries are mostly accidental gunshot wounds, that is not the case. The most common hunting injury in deer season is a fall from a tree stand.
Tree stands typically allow a hunter to perch 10 to 30 feet above the ground and wait for game to wander by. They are more frequently used in the South and Midwest, usually for deer hunting. A recent study by the Ohio State University Medical Center looked at hunting related injury patterns at two trauma centers.
Half of the patients with hunting-related injuries fell, and 92% of these were tree stand falls. Only 29% were gunshots. And unfortunately, alcohol increases the fall risk, so drink responsibly!
Most newer commercial tree stands are equipped with a safety harness. The problem is that many hunters do not use it. And don’t look for comparative statistics anytime soon. There are no national reporting standards. No matter how experienced you are, always clip in to avoid a nasty fall!
The image on top is a commercial tree stand. The image below is a do-it-yourself tree stand (not recommended). Remember: gravity always wins!


Thanks for reading!
Michael

Finding pneumomediastinum on a chest xray or CT scan always gets one’s attention. However, seeing this condition after a simple fall from standing is very simple to evaluate and manage.
There are 3 potential sources of gas in the mediastinum after trauma:
Blunt injury to the esophagus is extremely rare, and probably nonexistent after just falling down. Likewise, a tracheal injury from falling over is unheard of. Both of these injuries are far more common with penetrating trauma.
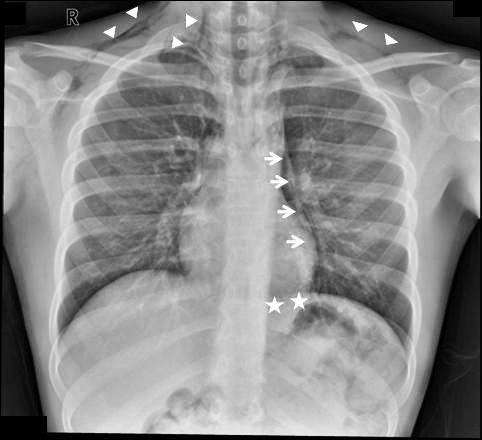
This leaves the lung and smaller airways within it to consider. They are, by far, the most common sources of pneumomediastinum. The most common pattern is that this injury causes a small pneumothorax, which dissects into the mediastinum over time. On occasion, the leak tracks along the visceral pleura and moves directly to the mediastinum.
Management is simple: a repeat chest xray after 6 hours is needed to show non-progression of any pneumothorax, occult or obvious. This image will usually show that the mediastinal air is diminishing as well. There is no need for the patient to be kept NPO or in bed. Monitor any subjective complaints and if all progresses as expected, they can be discharged after a very brief stay.
Tomorrow: A more interesting (and complicated) case of pneumomediastinum.