Here’s a very interesting case for you. A construction worker was carrying an object inside a building WHILE HOLDING HIS NAIL GUN! As he passed through the door, his elbow hit the frame and he brushed his neck with the business end of the gun. Guess what happened?
He experienced sharp pain, then noted pain every time he swallowed. He checked himself out in the mirror, and there was a small puncture wound in the right side of his neck. He presented to his local ED, with the complaints just noted. He was hemodynamically stable and neurologically intact. His airway was patent, and he had minimal pain. The following image was obtained. The nail measures about 6cm in length.
Let me know (by Twitter or comments) what additional information you think you need. I’ll discuss that in my next post. Then we’ll figure out what to do about this problem.
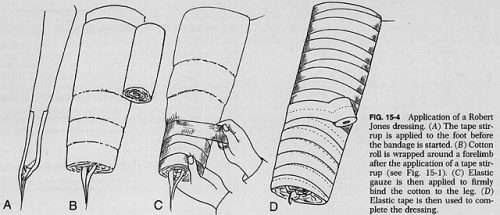
The Robert Jones dressing is a thick, padded bandage classically applied to the thigh and leg. It is thought to reduce swelling by applying even pressure to the extremity, which in turn should promote healing. And since it is a soft dressing, as opposed to a cast, there is less chance of developing skin breakdown from direct pressure. Here’s a compression-type dressing described in 1937 using stockinette, cotton wool, and elastic cloth, although it was not attributed to Jones at that point.
Charnley provided a detailed description of the bandage in 1950, and was the first to refer to Jones.
Interestingly, Robert Jones never really referred to the dressing by name. There were references to a “pressure crepe bandage over copious wool dressing” in his operative logs, but it wasn’t until much later that his name became associated with it. Because of this, the composition of the bandage has varied greatly over time.
But who was Robert Jones? We in the States are fairly ignorant, but my UK readers are very familiar. Jones was a British surgeon who practiced through the late 1800s and past the end of World War I. He learned about fractures from his uncle, and became one of the few surgeons of the time to be interested in fracture care. Until then, orthopaedics was focused primarily on correcting deformities in children. He received his FRCS in 1889. After being appointed Surgeon-Superintendent of the Manchester Ship Canal, he established the first comprehensive accident service in the world to take care of injured workers. He founded the British Orthopaedic Society in 1894, and introduced the concept of military orthopaedic hospitals during World War I. His innovations led to significant decreases in morbidity and mortality from fractures in the war, particularly of the femur.
And does his eponymous dressing actually work? There has been little research in this area. There is one study that I have found that actually measured compartment pressures to see if the loss of edema from compression caused a noticeable pressure decrease. Here are the factoids:
This was a very small prospective study from 1986 of 9 patients (!) who had just undergone knee arthroplasty
Slit catheters were placed into the compartment 10 cm below the knee joint (but they didn’t say which compartment)
Thick cotton-wool from a roll was applied over the surgical dressings twice, each with a thickness of two inches. An elastic bandage was then applied snugly.
Much to the researchers’ surprise, compartment pressures did not fall as expected over time. They were basically constant until the dressing was removed. Then the pressures fell significantly.
Bottom line: Robert Jones’ fame is well deserved. However, his dressing (which he did not name, and may not even be what he used), did not have the pressure-reducing effect on an injured limb that surgeons thought. No studies on edema and healing have been done. It’s basically a fluffy dressing. However, that is a good thing. It keeps the leg padded, protecting the skin, and immobilized. It’s like a very well padded cast, without the risk of skin breakdown. And because of its simplicity, it will probably be used for quite some time to come.
References:
The Robert Jones bandage. JBJS 68B(5):776-779, 1986.
The treatment of fracture without plaster of Paris. Closed Treatment of Common Fractures, E&S Livingstone 1950, pg 28-29.
Handbook of Orthopaedic Surgery. CV Mosby 1937, pg 418.
How long does it take for EMS to get to the scene of an emergency? That’s a loaded question, because there are many, many factors that can impact this timing. If you look at the existing literature, there are few, if any, articles that have actually looked at this successfully.
A group from Aurora, IL and Wake Forest reviewed EMS records from across the country, spanning 485 agencies over a one year period. Only 911 responses were reviewed, and outliers with arrival times of more than 2 hours and transport times of 3 hours were excluded. Over 1.7 million records were analyzed, and 625 were excluded for this reason.
Here are the factoids:
In 71% of cases, the patient was transported to a hospital. In one quarter of cases, they were evaluated but not transported. 1% were dead on arrival, and in 2% no patient was found at the scene (!)
4% of patients were transported in rural zip codes, 88% in suburban ones, and 8% from urban locations
Overall response time averaged 7 minutes
Median response times were 13 minutes for rural locations, and 6 minutes for both suburban and urban locations
Nearly 1 in 10 patients waited 30 minutes for EMS response in rural locations
Bottom line: There is an obvious difference in EMS response times between rural and urban/suburban locations. And there are many potential reasons for this, including a larger geographic area to be covered, volunteer vs paid squads, etc. Many of these factors are difficult, if not impossible to change. The simple fact that it takes longer to reach these patients increases their potential morbidity and mortality. Remember, time is of the essence in trauma. The patient is bleeding to death until proven otherwise. It is far easier and cost-effective to equip bystanders with the skills to assist those in need (basic first aid, CPR, Stop the Bleed, etc) while waiting for EMS to arrive.
Reference: Emergency Medical Services Response Times in Rural, Suburban, and Urban Areas. JAMA Surg 152(10): 983–984, 2017.
The July Trauma MedEd Newsletter is now available! It provides information on producing an Advanced Trauma Life Support (ATLS) course in the times of the Coronavirus. It describes how to adhere to various safety guidelines and details the technology needed to pull it off.
Trauma education has gotten significantly more difficult in the face of the Coronavirus. In-person education offerings like ATLS and PALS courses, TNCC courses, and major trauma conferences are routinely being cancelled or delayed. And many of them have decided to move to a virtual format.
Until early this year, I traveled around the country as a speaker for numerous trauma education conferences. The bulk of these have been cancelled for the remainder of the year. A few have opted to try an online format, and I will be giving several online talks in the coming months.
The American Association for the Surgery of Trauma (AAST) has converted their physical meeting in Hawaii to a virtual one (sigh). I will definitely be participating anyway!
Here are two conferences I will be speaking at, using the new virtual format. If you are in need of some quality education, check them out:
Virtual Excellence in Trauma Care Conference
Intermountain Medical Center – Salt Lake City UT
September 17-18, 2020
Presentations:
1. Keynote Address: Massive Bleeding Associated With Pelvic Fractures
2. Trauma Mythbusters
Registration Info: click here
Brochure: click here
Stormont Vail Trauma Symposium Stormont Vail Hospital – Topeka KS
October 16, 2020
Presentations:
1. New Trends in Trauma
2. Mobility of the Trauma Patient in ICU
Registration and brochure: available soon
And if your hospital or organization is interested in putting your own grand rounds or other educational conference together, I am now focusing on providing presentations via telepresence.
Granted, telepresence is not the same as being there in person. It’s so much nicer to meet people in person, and it’s much more satisfying to make that more personal connection. But in-person conferences won’t be in the cards for a while. In the meantime, I hope to see you all soon via WebEx or Zoom! Please reach out!
Home of the Trauma Professional's Blog
Do you want to get a daily email every time there’s a new post? See what I’m up to.