Last week, I published a preliminary practice guideline for nonoperative management of abdominal stab wounds. Click here to view it. A key part of that guideline is the serial abdominal exam. Surgeons talk about this a lot, but how do you do it? I posted about many of the details here.
The serial exam is nuanced enough so that it deserves its own clinical practice guideline! You won’t find this in any doctor or nursing books. It’s really simple, but the devil is truly in the details.
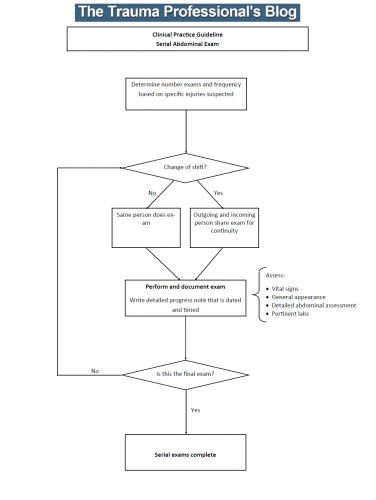
Click this image or the link below to download the guideline. I’ve also posted a Microsoft publisher version in case you want to modify it to suit your center.
Please feel free to email or post comments and questions in the area below this post!
References:
How often have you seen this in an admitting history and physical exam note? “Admit for observation; serial abdominal exams.” We say it so often it almost doesn’t mean anything. And during your training, did anyone really teach you how to do it? For most trauma professionals, I believe the answer is no.
Yet the serial abdominal exam is a key part of the management of many clinical issues, for both trauma patients as well as those with acute care surgical problems.
Here are the key points:
- Establish a baseline. As an examiner, you need to be able to determine if your patient is getting worse. So you need to do an initial exam as a basis for comparisons.
- Pay attention to analgesics. Make sure you know what was given last, and when. You do not need to withhold pain medications. They will reduce pain, but not eliminate it. You just need enough information to determine if the exam is getting worse with the same amount of medication on board.
- Perform regular exams. It’s one thing to write down that serial exams will be done, but someone actually has to do them. How often? Consider how quickly your patient’s status could change, given the clinical possibilities you have in mind. In general, every 4 hours should be sufficient. Every shift is not. And be thorough!
- Document, document, document. A new progress note should be written, dated and timed, every time you see your patient. Leave a detailed description of how the patient looks, vital signs, pertinent labs, and of course, exact details of the physical exam.
- Practice good handoffs. Yes, we understand that you won’t be able to see the patient shift after shift. So when it’s time to handoff, bring the person relieving you and do the exam with them. You can describe the pertinent history, the exam to date, the analgesic history, and allow them to establish a baseline that matches yours. And of course, make sure they can contact you if there are any questions.
Home of the Trauma Professional's Blog