I’ve written a lot about chest tubes, but there’s actually a lot to know. And a fair amount of misinformation as well. Here’s some info you need to be familiar with:
I’ve written a lot about chest tubes, but there’s actually a lot to know. And a fair amount of misinformation as well. Here’s some info you need to be familiar with:
- Chest trauma generally means there is some blood in the chest. This has some bearing on which size chest tube you choose. Never assume that there is only pneumothorax based on the chest xray. Clot will plug up small tubes.
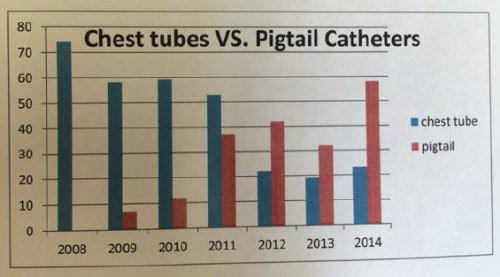
- Chest tubes for trauma only come in two sizes: big (36Fr) and bigger (40Fr). Only these large sizes have a chance in evacuating most of the clot from the pleural space. The only time you should consider a smaller tube, or a pigtail type catheter, is if you know for a fact that there is no blood in the chest. The only way to tell this is with chest CT, which you should not be getting for diagnosis of ordinary chest trauma. Having said this, there is some more recent literature that suggests that size might not matter as much as we think.
- When inserting the tube, you have no control of the location the tube goes once you release the instrument used to place it. Some people believe they can direct a tube anteriorly, posteriorly, or anywhere they want. They can’t, and it’s not important (see next tip).
- Specific tube placement is not important, as long as it goes in the pleural space. Some believe that posterior placement is best for hemothorax, and anterior placement for pneumothorax. It doesn’t really matter because the laws of physics make sure that everything gets sucked out of the chest regardless of position except for things too big to fit in the tube (e.g. the lung).
- Tunneling the tube tract over a rib is not necessary in most people. In general, we have enough fat on our chest to ensure that the tract will close up immediately when the tube is pulled. A nicely placed dressing is your insurance policy.
- Adhere to an organized tube management protocol to reduce complications and the time the tube is in the chest.
And finally, amaze your friends! The French system used to size chest tubes is the diameter of the tube in millimeters times three (3.14159, pi to be exact). So a 40Fr chest tube has a diameter of 13.3mm.