Here’s a 9 minute video demonstrating my easy technique for inserting a chest tube. I’ve included some helpful tips and tricks to make this a quick and easy procedure.


Here’s a 9 minute video demonstrating my easy technique for inserting a chest tube. I’ve included some helpful tips and tricks to make this a quick and easy procedure.
 I’ve written a lot about chest tubes, but there’s actually a lot to know. And a fair amount of misinformation as well. Here’s some info you need to be familiar with:
I’ve written a lot about chest tubes, but there’s actually a lot to know. And a fair amount of misinformation as well. Here’s some info you need to be familiar with:
And finally, amaze your friends! The French system used to size chest tubes is the diameter of the tube in millimeters times three (3.14159, pi to be exact). So a 40Fr chest tube has a diameter of 13.3mm.
I’m dedicating the coming fortnight (that’s two weeks to you non-Brits) to the lowly chest tube. It’s taken for granted, but there is a lot a variability on how we insert, manage, and pull out these devices. Here’s what’s coming, starting tomorrow:
If you want email reminders every day when a post goes live, just click here to subscribe!
Over the last three days, I reviewed some data on lytics at the request of some of my readers. Then I looked at a paper describing one institution’s experience dealing with retained hemothorax, including the use of VATS. But there really isn’t much out there on how to roll all this together.
Until now. The trauma group at Vanderbilt has a paper in press describing their experience with a home-grown practice guideline for managing retained hemothorax. Here’s what it looks like:
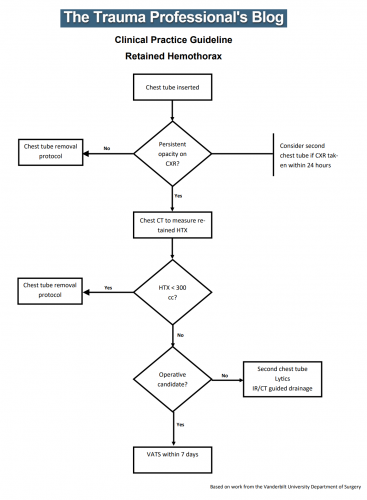
I know it’s small, so just click it to download a pdf copy. I’ve simplified the flow a little as well.
All stable patients with hemothorax admitted to the trauma service were included over a 2.5 year period. The practice guideline was implemented midway through this study period. Before implementation, patients were treated at the discretion of the surgeon. Afterwards, the practice guideline was followed.
Here are the factoids:
Bottom line: This is how design of practice guidelines is supposed to work. Identify a problem, typically a clinical issue with a large amount of provider care variability. Look at the literature. In general, find it of little help. Design a practical guideline that covers the major issues. Implement, monitor, and analyze. Tweak as necessary based on lessons learned. If you wait for the definitive study to guide you, you’ll be waiting for a long time.
This study did not significantly change outcomes like hospital stay or complications. But it did decrease the number of more invasive procedures and decreased variability of care, with the attendant benefits from both of these. It also dictates more selective (and intelligent) use of additional tubes, catheters, and lytics.
I like this so much that I plan to adopt it at my center!
Download the practice guideline here.
Related posts:
Posts in this series:
Reference: Use of an evidence-based algorithm for patients with traumatic hemothorax reduces need for additional interventions. J Trauma, in press, December 14, 2016.
I’ve written about the use of lytics to treat retained hemothorax over the past few days. Although it sounds like a good idea, we just don’t know that it works very well. And they certainly don’t work fast. Lengths of stay were on the order of two weeks in both studies reviewed.
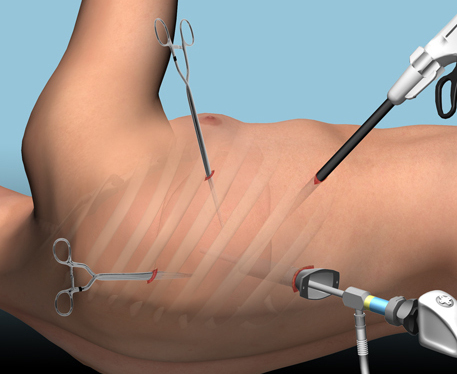
The alternative is video assisted thoracoscopic surgery (VATS). So let’s take a look at what we know about it. This procedure is basically laparoscopy of the chest. A camera is inserted, and other ports are added to allow insertion of instruments to suck, peel, and scrape out the hemothorax.
A prospective, multi-center study was performed over a 2 year period starting in 2009. Twenty centers participated, contributing data on 328 patients with retained hemothorax. This was defined as CT confirmation of retained blood and clot after chest tube placement, with evidence of pleural thickening.
Here are the factoids:
Bottom line: There’s a lot of data in this paper. Most notably, many patients resolve their hemothorax without any additional management. But if they don’t, additional tubes, guided drain placement, and lytics work only a third of the time and contribute to additional time in the hospital. Even VATS and thoracotomy require additional maneuvers 20-30% of the time. And infectious complications are common. This is a tough problem!
Tomorrow, I’ll try to roll it all together and suggest an algorithm to try to optimize both outcomes and cost.
Posts in this series:
Reference: Management of post-traumatic retained hemothorax: A prospective, observational, multicenter AAST study. 72(1):11-24, 2012.