Cervical spine clearance is another one of those tasks that everyone seems to do their own way. Most trauma centers have an algorithm for clearance, or even two, like my center. But anytime different clinicians or centers do the same thing in different ways, it means we don’t really know what we’re doing.
It basically means that the hard data is not there to dictate what we truly should do. So there are two alternatives:
- Wait for good data to become available. Unfortunately, this can take forever.
- Extrapolate from any existing data, and fill in the gaps with our clinical experience to come up with something that works and causes no harm.
The protocols in use at Regions Hospital are based on #2, and have been in place for over a decade. But now, we have a good example of #1 to work with.
Fortunately for us, cervical spine clearance has been evolving for decades. And as technology has improved, so has our ability to miss fewer and fewer “significant” injuries. A multi-center trial published this month provides one of the final puzzle pieces to help us settle upon a uniform cervical spine clearance guideline. It was a prospective look at intoxicated patients after blunt trauma, who can’t always participate in the process of clinical cervical spine clearance.
This three year study took place at 17 centers and specifically looked at the combination of clinical and radiographic clearance in alcohol and drug intoxicated patients. Over 10,000 patients participated in the study. There are some limitations, of course, when so many centers participate. But the pros massively outweigh the cons.
Here are the factoids:
- The overall incidence of cervical spine injury was 10.6% (!)
- 30% of patients were intoxicated (19% etoh, 6% drugs, 5% both (also !)
- Intoxicated patients had a significantly lower incidence of cervical injury (8% vs 12%). (Don’t get any ideas about the old adage about being relaxed when they crash. This probably represents lower speeds involved.)
- For intoxicated patients, sensitivity of CT scan was 94%, specificity was 99.5%, and the negative predictive value (NPV) was 99.5%
- The NPV for clinically significant injuries in intoxicated patients was 99.9%, and no unstable injuries were missed by CT (100% NPV) (!!)
- When CT was negative, being intoxicated led to longer time in a collar (8 hrs vs 2 hrs)
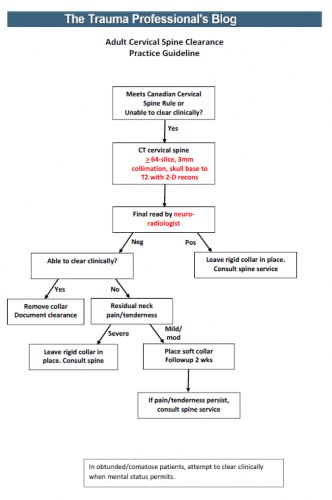
Bottom line: Fear of clearing the cervical spine without a clinical exam, or in obtunded or intoxicated patients, is primarily due to old anecdotal reports. And much of it is not first-hand experience, but rumors of others’. What is finally becoming clear is that it is okay to clear based upon radiographic findings alone.
Tomorrow, I’ll provide my version of a new, unified clearance protocol based on this work.
Reference: Cervical spine evaluation and clearance in the intoxicated patient: A prospective Western Trauma Association Multi-Institutional Trial and Survey. J Trauma 83(6):1032-1040, 2017.