Our current technology for identifying venous thromboembolism (VTE) / deep venous thrombosis (DVT) consists of duplex ultrasonography, and sometimes, CT angiography. Both are relatively noninvasive and painless (unlike the old-fashioned venography of days gone by.
Researchers at the Massachusetts General Hospital have been working with different chemical probes that could adhere to clot and allow it to be identified on a PET scan. After experimenting with a number of fibrin-targeting peptides they settled upon one called copper fibrin-binding peptide 8 (Cu-FBP8). It was found to have a high affinity for clot, remain stable, and clear quickly from the animal.
A series of rats were subject to a surgically induced thrombus in the carotid or femoral arteries, or a sham operation. The animals were then imaged by CT/PET scan after injection with the Cu-FBP8 probe. The authors found that the probe worked as expected, identifying clot immediately. They were also able to follow resolution over the days following induction.
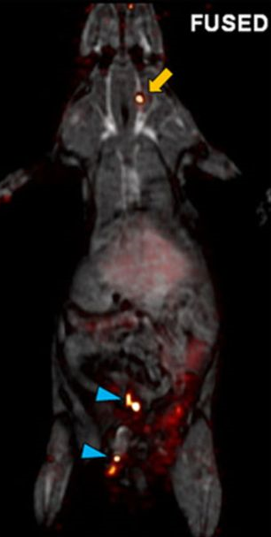
Here is a whole-body fused CT/PET scan of one of the animals with both carotid artery (yellow arrow) and femoral artery (blue arrows) clot.
Bottom line: This is a potentially exciting tool that could make it much easier for us to identify DVT and VTE. It could also help us understand the etiology and incidence of PE as well. But as with all animal studies, it remains to be seen whether this will translate into a useful test for humans. Stay tuned, as it will probably take about 3 years to find out the answer.
Reference:
Multisite Thrombus Imaging and Fibrin Content Estimation With a Single Whole-Body PET Scan in Rats. Arterioscler, Thromb, Vasc Biol 35(10):2114-2121, 2015.