Trauma hurts like hell. Over the years, we’ve developed quite a few ways of combating this pain. A number of drug classes have been developed to reduce it. One of the more common non-narcotic drug classes are the NSAIDs. As I’ve mentioned before, every drug has dozens of effects. Drug companies market a particular medication based on one of the predominant effects. All the others are considered side effects.
NSAIDs are not unique; they have lots of side effects as well. In 2003, several papers brought to light possible interactions between these drugs and fracture healing. Specifically, there were questions about these drugs interfering with the healing process and of increasing the number of delayed unions or nonunions. But once again, how convincing were these papers, really?
It would seem to make sense that NSAIDs could interfere with bone healing. This process relies heavily on the regulation of osteoblast and osteoclast function, which itself is regulated by prostaglandins. Since prostaglandins are synthesized by the COX enzymes, COX inhibitors like the NSAIDs should have the potential to impair this process. Indeed, animal studies in rats and rabbits seem to bear this out.
But as we have seen before, good animal studies don’t always translate well to human experience. Although a study from 2005 suggested that NSAID administration in older patients within 90 days of injury had a higher incidence of fracture nonunion, the study design was not a very good one. It is equally likely that patients who required these drugs in this age group may have been at higher risk for nonunion in the first place.
In fact, there are no large, prospective randomized studies that have explored the effect of short-term or long-term NSAID administration on fracture repair. But there have been several smaller studies that showed absolutely no effect on nonunion with short-term administration of this drug class. Yet the dogma that leads us to avoid giving these drugs persists.
A recent analysis looked at the quality of the published research, both for and against NSAID usage in fracture patients. They used the Coleman Methodology Score, which evaluates study size and type, mean followup, detailed description of treatment, subject selection, outcomes, and outcome assessment. The maximum score was 100.
Here are the factoids:
- There were 4x as many total subjects in the “NSAIDS are okay” papers than in the “avoid NSAIDS” papers
- The quality of the “NSAIDS are okay” papers were significantly higher than “avoid NSAIDS” group (59 vs 40)
- Interestingly, the “avoid NSAIDS” papers are cited twice as often
- All of the reviews ended with my pet peeve catch phrase “further (good) research is needed”
Bottom line: Once again, the animal data is clear but the human data is not. Although there are theoretical concerns about their use, there is not enough solid risk:benefit information to abandon short-term NSAID use in patients who really need them. NSAIDs can and should be prescribed in patients with short-term needs and simple fractures.
References:
- Effects of nonsteroidal anti-inflammatory drugs on bone formation and soft-tissue healing. J AM Acad Orthop Surg 12:139-43, 2004.
- Effect of COX-2 on fracture-healing in the rat femur. J Bone Joint Surg Am 86:116-123, 2004.
- Effects of perioperative anti-inflammatory and immunomodulating therapy on surgical wound healing. Pharmacotherapy 25:1566-1591, 2005.
- Pharmacological agents and impairment of fracture healing: what is the evidence? Injury 39:384-394, 2008.
- High dose nonsteroidal anti-inflammatory drugs compromise spinal fusion. Can J Anaesth 52:506-512, 2005.
- Nonsteroidal Anti-Inflammatory Drugs and Bone-Healing: A Systematic Review of Research Quality. JBJS Rev 4(3), 2016.

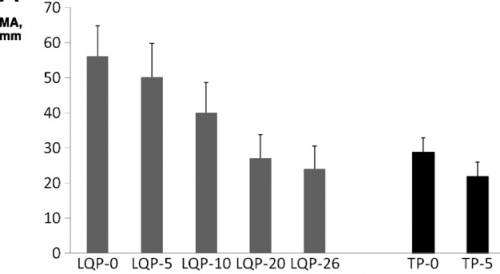 (TEG MA for liquid (LQP) and thawed (TP) plasma
(TEG MA for liquid (LQP) and thawed (TP) plasma