In 2009, the Health Information Technology for Economic and Clinical Health (HITECH) act was passed. This provided an incentive for all US hospitals to demonstrate “meaningful use” of the EHR. For those of you interested in the details, check out the related post link at the end of this article.
Hospitals rushed to comply, shelling out lots of money to try to recoup some of it through these incentives. In theory, using an EHR should allow better record sharing, increase patient satisfaction, reduce unnecessary testing and medical errors, and ideally, improve billing. But does it work?
A community hospital with a medium-sized ED looked at physician productivity in the ED while using an EHR. In this case, the software product was McKesson, and 16 clinicians were monitored prospectively over a 30 hour period.
Here are the factoids:
- The group consisted of attending physicians, residents, and nurse practitioners / physician assistants
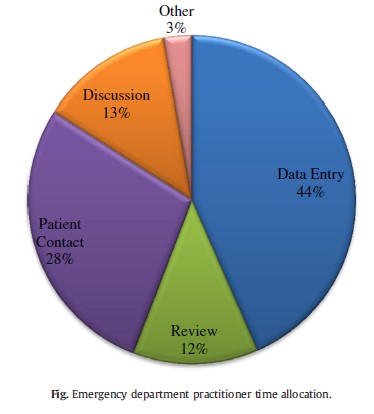
- The distribution of how they spent their time is shown below:
- In order to complete an assessment in the EMR, it took an average of 160 mouse clicks
- On average, clinicians saw 2.12 patients per hour, requiring nearly 4000 mouse clicks to complete their charting
Bottom line: Overall, this is not a very good or coherent or even well-designed study. But it does show us one thing. Clinicians spent only 28% percent of their time seeing patients, and 56% of their time reviewing or entering data into the EHR! Note the blue and green wedges in the pie chart. How can they possibly earn their salaries? Other studies have confirmed that using an EHR does decrease throughput slightly, yet reimbursements increase anyway.
How can this be? EHRs were originally designed to facilitate billing, and it looks like they still do, making up for the fact that fewer patients can be seen. But this seems like a perverse incentive to me. Adopt the EHR, see fewer patients, get paid more!?
Related posts:
Reference: 4000 Clicks: a productivity analysis of electronic medical records in a community hospital ED. Am J E Med 31:1591-1594, 2013.