So what is going on with your dyspneic patient after partial ejection from their car? They are not responding to your interventions as they should How is he immune to chest tube placement?
Well, you could intubate the patient. But the x-ray will be available momentarily, and may guide you along a different path. It might even obviate the need for intubation. So while you are getting your meds ready (just in case), this image comes up:
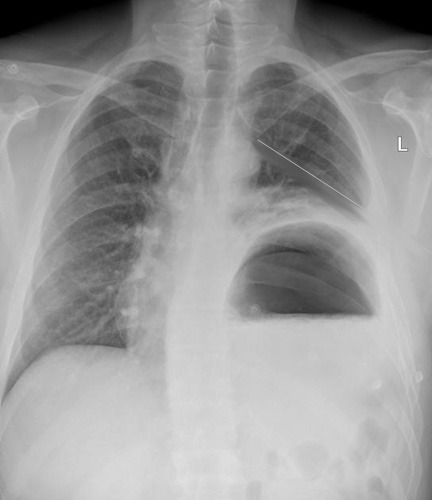
The chest tube is in good position, but the stomach is not!
The reason your patient didn’t respond to the chest tube is that they have a traumatic rupture of the diaphragm with the stomach in the chest. It is compressing a good portion of the left lung, leading to dyspnea and poor oxygen saturation.
Rapidly place a nasogastric tube to try to decompress the stomach. It doesn’t always work because the angles at the hiatus are not what they usually are. But if it does, the patient will feel better immediately. You may be able to avoid intubating them… for a few minutes. This is a surgical problem, and commonly involves injury to other abdominal structures, especially the spleen. Order up some blood, and rapidly complete your evaluation. A pelvis x-ray is in order, because fractures are common after full or partial ejection through the window. No other imaging is necessary. The send your patient off to the OR for a thorough exploration and repair. Now you can intubate.
I’ve seen this injury three times after partial ejection, and always involving the driver (left side, makes sense). Any time you have left sided abnormalities after blunt trauma that don’t respond to a chest tube, think about this problem.


