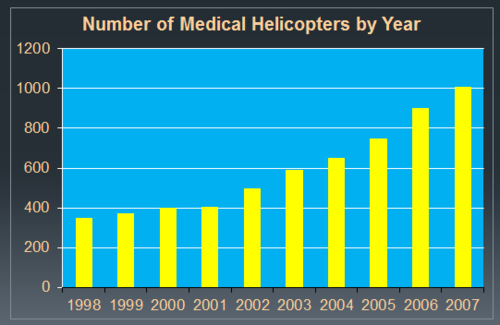
There has been tremendous debate around the value and use of prehospital helicopter emergency medical services (HEMS). It’s fast, but also expensive, and there is always a small amount of added risk to patients during transport. Over the years, there has been a significant increase in the number of helicopter services, and in some cases it seems like several services are dashing to accident scenes in the hope that they can pick up the patient.
Overuse of HEMS has also been recognized, with some patients transported who could have just as easily and safely been moved by ground ambulance. This is a particularly vexing problem with pediatric patients.
The holy grail of trauma HEMS has been to find some easy to identify scene variables that reliably predict which patients should be transported by air. A group in North Carolina tapped the state trauma registry to attempt to develop such a system. They analyzed data in the registry over a three year period, mathematically analyzing for easily identified predictors of ED death or need for operating room, interventional radiology, or ICU admission.
Here are the factoids:
- The percentage of flights from the scene increased from 7% to 9% compared to data from fifteen years prior to this study
- Vital signs (SBP, pulse, GCS motor) had the best correlation with mortality, and these were used to develop a regression model for triage
- Patients with normal SBP, pulse, and GCS motor of 6 were found to safely transported by ground EMS, with similarly low mortality for ground or air
- During the study period, triaging patients that met these criteria would have saved the state system about $19 million
Bottom line: Every state should take a look at their guidelines for helicopter vs ground transport for scene runs. This is an expensive tool, and should be treated with respect. Just because a helicopter is available does not mean it should be used. The commander on the scene must make the proper decision based on variables like these, but also apply their knowledge of traffic patterns, time and distance from the most appropriate receiving trauma center.
Reference: Trauma system resource preservation: a simple scene triage tool can reduce helicopter emergency medical services (HEMS) over-utilization in a state trauma system. Session IV Paper 13, AAST 2018.