One of the big unanswered questions in the management of pneumothorax is, how big is too big? At what size is a chest tube of some type mandatory?
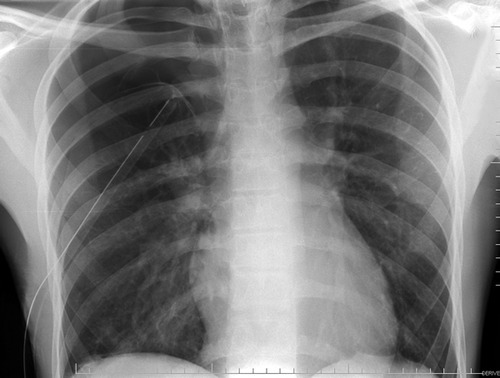
The problem is that we just don’t have any good data. Seems like a simple problem, right? Unfortunately, it’s not. A pneumothorax is a three dimensional collection that surrounds the lung in very random ways. All we had to detect and “measure” them for decades was the lowly chest x-ray. Unfortunately, this is a 2D shadow picture that does not allow us to accurately estimate the size.
A few old papers exist that tried to quantify pneumothorax, but they are of no use now that we have chest CT. Unfortunately this new technology has drawbacks, as well. First, it’s just a stack of 2D images that our minds assemble into a 3D mental model, so it’s still difficult to quantify the air. And second, you shouldn’t be getting a chest CT just to diagnose pneumothorax. In blunt trauma, it’s really just for checking the thoracic aorta for injury.
So we’re left with the original question, and there are three answers. If there is any physiologic compromise (hypoxia, tachypnea, anxiety), then the chest should be drained. If the pneumothorax is enlarging over serial chest x-rays, then it should be drained before it causes physiologic change. And finally, if there is concern that it is so large that it will take too long to absorb, especially in older patients with comorbidities, a chest drain should be inserted. This is a somewhat soft indication, however.
Bottom line: The three reasons above are the usual answers to the question, “how big is too big?” For me, once the pneumothorax pushes the lung 1-2 cm away from the chest wall from apex to base, it’s time for a tube.
Related posts: