The Eastern Association for the Surgery of Trauma (EAST) has been at the forefront of trauma practice guideline dissemination for decades. They recently published a set of recommendations for managing patients with bladder injury. These injuries are not commonly encountered by trauma professionals, and I thought a refresher on current thinking on their management was in order.
Using the usual methodology, the trauma literature was scanned for papers dealing with this topic. After screening for quality, the field was narrowed to 17 papers which were used to formulate the published recommendations. These cover imaging and management questions that frequently come up during the evaluation of these patients.
Following are the questions raised, the EAST recommendations, and my commentary about them:
-
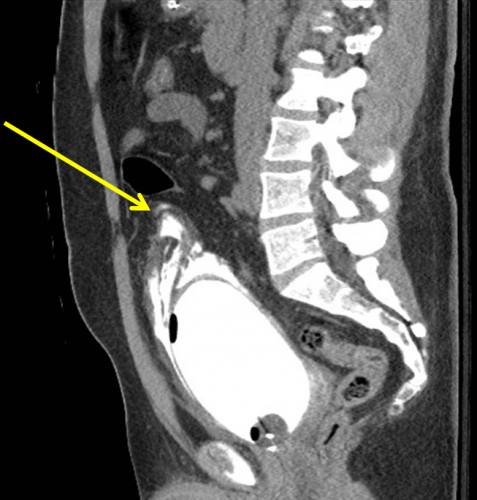
- In patients with abdominal / pelvic trauma, should retrograde CT cystography vs no imaging be used to diagnose a bladder injury? This seems like a silly question, but the answer lies in the details. It all boils down to the likelihood of injury. And how does one determine likelihood? By looking at the urine and the fracture patterns around the bladder. Patients with microscopic hematuria are very unlikely to have a bladder injury, and any type of bladder imaging in these patients (cystogram, CT cystogram) is almost never positive, and so is not indicated. This is the reason that ordering a urinalysis in major trauma patients is not recommended. However, if gross hematuria is present, CT cystogram is recommended. The sensitivity and specificity are nearly perfect. Just be sure to do a true cystogram by actively filling the bladder with contrast via a urinary catheter. Passive filling of the bladder with urine from the IV contrast misses about half of all the injuries. Also, strongly consider adding CT cystogram in patients with widening of the pubic symphysis. This injury pattern is frequently associated with bladder injury.
- In patients with intraperitoneal bladder rupture from blunt trauma, should operative or nonoperative management be used to decrease complications? Another silly question? In general, intraperitoneal bladder ruptures do not heal on their own, so urine continues to bathe the peritoneal cavity until the injury is fixed. The review article recommended that operative repair be performed in all of these cases.
- In patients with extraperitoneal bladder rupture from blunt trauma, should operative or nonoperative management be used to decrease complications? Patients with a simple extraperitoneal bladder injury should undergo nonoperative management. These injuries usually heal and seal within about 10 days. However, patients with this type of bladder injury that is more complicated (bone spicules piercing the bladder, concomitant vaginal or rectal injury, bladder neck injury) should undergo operative repair in order to decrease the complication rate. One additional group that should be repaired: patients with pubic diastasis that will require operative fixation. The bladder should be repaired at the time of the orthopedic procedure to avoid bathing the new hardware in urine.
- In patients who have undergone operative or nonoperative management of bladder injury, should bladder closure be assessed with cystogram or not? This one depends on the type and complexity of injury. For simple intraperitoneal bladder injuries that were operatively repaired, no followup cystogram is required. More complex repairs should be evaluated by cystogram before removing the urinary catheter. Finally, simple extraperitoneal injuries should also have a cystogram obtained before removing the catheter. My magic number for obtaining followup studies is 10 days. There is no real science behind this, and no one has systematically looked at 5 vs 7 vs 10 vs 14 days. This one is based only on personal experience.
And by the way, most simple bladder injuries (both intra- and extra-peritoneal) can be easily repaired using two layers by your friendly neighborhood trauma surgeon. More complex injuries are generally best left to the urologist.
Reference: Management of blunt force bladder injuries: A practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma 86(2):326-336, 2019.