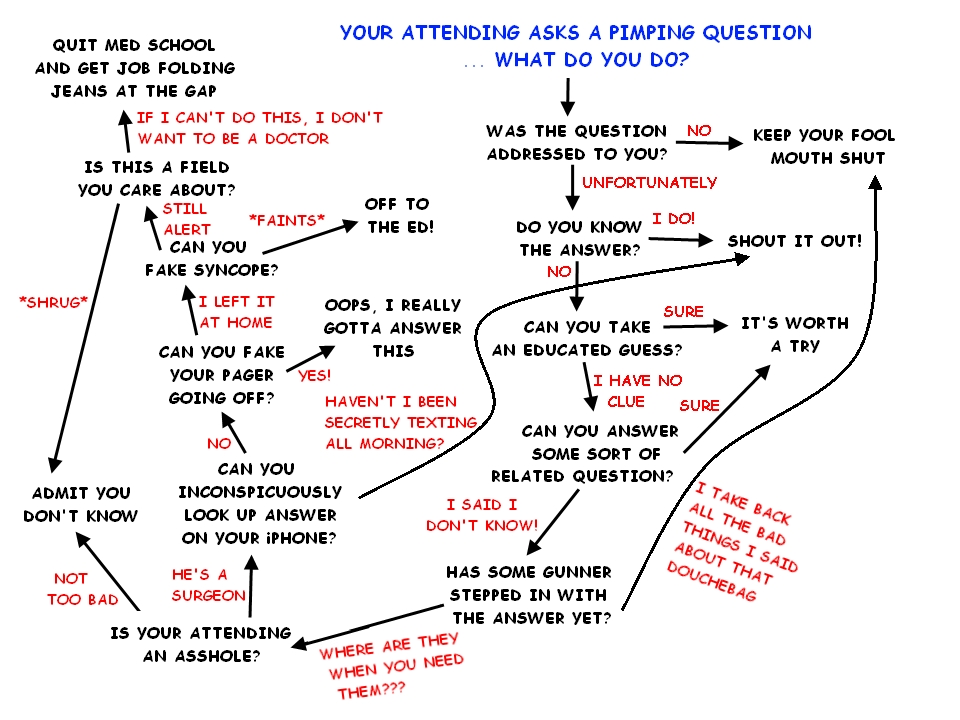
You know what I’m talking about. It’s a mainstay of medical education for physicians. It starts in medical school, and generally never stops. And when you finish your residency, you graduate from being pimped to being the pimper.
How did this all come to be? Is it good for education? Bad? Tune in tomorrow to learn more. In the meantime, enjoy this algorithm on how to get through a pimping session. Click to view full-size.

Source: Posted by Dr. Fizzy on The Almost Doctor’s Channel
You know what I’m talking about. It’s a mainstay of medical education for physicians. It starts in medical school, and generally never stops. And when you finish your residency, you graduate from being pimped to being the pimper.
How did this all come to be? Is it good for education? Bad? Tune in tomorrow to learn more. In the meantime, enjoy this algorithm on how to get through a pimping session. Click to view full-size.
Source: Posted by Dr. Fizzy on The Almost Doctor’s Channel
You know what I’m talking about. It’s a mainstay of medical education for physicians. It starts in medical school, and generally never stops. And when you finish your residency, you graduate from being pimped to being the pimper.
How did this all come to be? Is it good for education? Bad? Tune in tomorrow to learn more. In the meantime, enjoy this algorithm on how to get through a pimping session. Click to view full-size.
Source: Posted by Dr. Fizzy on The Almost Doctor’s Channel
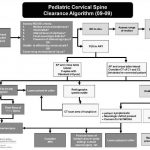
Algorithm For Clearing the Pediatric Cervical Spine
I previously wrote about a straightforward way to clear the cervical spine in children. Click here to see the article. Alfred I. DuPont Children’s Hospital has condensed their clearance technique into a relatively simple algorithm that can be used in conjunction with my previous tips.
Some notes on this algorithm:
- Can be performed only by attending physicians or a trauma resident in consultation with the attending trauma surgeon
- Clinical clearance alone may be carried out in select cases
- If radiographs are required, cross-table lateral, anterior/posterior, and odontoid views should be obtained (age 8 and above, non-intubated)
- Flexion / extension views should only be ordered in consultation with neurosurgery
Download a print version of the protocol here
Related post: How Do I Clear The Pediatric Cervical Spine?
Image and protocol courtesy of the Alfred I DuPont Children’s Hospital
Home of the Trauma Professional's Blog