It appears that no one was able to figure this one out! To recap, a young person (female in this case) sustained blunt trauma to the head. When her head was scanned, the following was found on the scout scan:
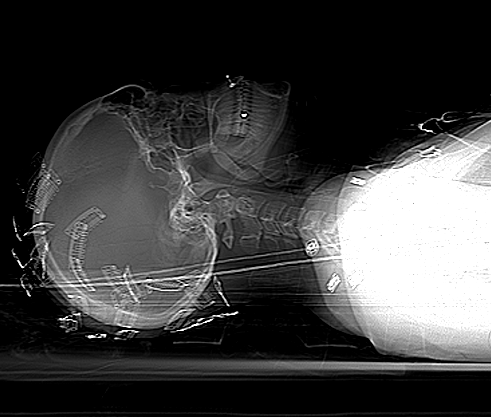
What is all this odd stuff? They look like some kind of metallic clips placed all over the head. The answer? Hair extensions! Here’s what they look like up close.

Unfortunately, they cannot be left in place during the CT. The amount of scatter is significant enough to degrade the quality of the study. By definition, if you have taken your patient to CT, they are stable and you have a little time. So carefully remove all of the extensions and place them in a bag and save them for the patient (they can be expensive!).
Make sure the CT tech obtains another topogram to confirm removal of all of the extensions. Then proceed with your CT as usual!