Need CPR? There’s An App For That!
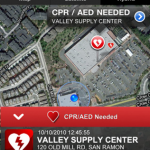
The San Ramon Valley Fire Protection District has released an iPhone app that gives users a window into their 911 dispatch center. When you install the app, you can indicate that you are trained in CPR. Your phone then provides your GPS location, and you can be notified of any sudden cardiac arrest events in your area. You can then proceed to the incident and render assistance, if appropriate.
App users can view all active incidents and the status of dispatched units. If an ambulance passes you or you are stuck in a traffic jam, just tap the screen to find out the details. They can also be notified of incidents by type, and monitor live emergency radio traffic.
The only downside is that leaving GPS location apps active in the background can significantly shorten your battery life. I think we can expect more communities to begin offering services like this in the near future.