Rapid infusion systems of some type are available in most EDs. However, this equipment is not routinely available in the field or in ground ambulances. Here’s a creative way to fashion one in a pinch for my overseas readers.
Note: The system described relies on an IV infusion set called the Intrafx SafeSet, available in Europe. The drip chamber in this set has a hydrophilic filter membrane integrated into the drip chamber that prevents air from passing through. This is critical for avoiding air embolism. Any product that traps air bubbles will work.
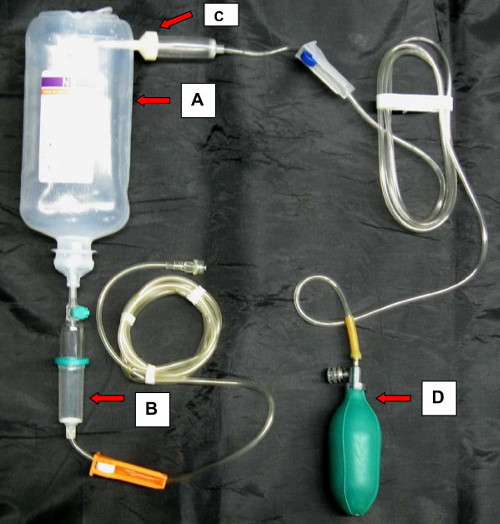
Here are the key components:
A – a fluid bottle with your choice of resuscitation fluid
B – an Intrafix SafeSet, or other drip chamber containing an air trap
C – another infusion set, spiked into A to pressurize it
D – a bulb from a sphygmomanometer for pressurizing A
Bottom line: This barebones, low cost rapid infuser can be used in hostile environments and can achieve rapid flow rates. But remember, the drip chamber (B) must be of an air-trapping type!
Reference: Novel rapid infusion device for patients in emergency situations. Scand J Trauma Resus Emerg Med 19:35, 2011.
Ever been in a trauma activation where it seems like the first thing that happens is that someone steps up to the patient with the ultrasound probe in hand? And then it takes 5 minutes of pushing and prodding to get the exam done?
Well, it’s not supposed to be that way. The whole point of adhering to the usual ATLS protocol is to ensure that the patient stays alive through and well after your exam. And FAST is not part of the primary or secondary surveys, it is an adjunct.
As always, there are a few exceptions to the rule above.
If an unstable patient arrives without an obvious source of bleeding, FAST of the abdomen should be able to detect if a large hemoperitoneum is present. This will expedite the patient’s transfer to the OR.
A patient in cardiac arrest may benefit from a quick FAST to determine if cardiac activity is present. If not, it may be time to terminate resuscitation.
Bottom line: With the exceptions noted above, always complete the ATLS primary and secondary surveys first. Then pull out the ultrasound machine, but be quick about it. If it takes more than about 60 seconds to do the exam, someone probably needs a little more practice.
The radiologist made me order that (unnecessary) test! I’ve heard this excuse many, many times. Do these phrases look familiar?
… recommend clinical correlation
… correlation with CT may be of value
… recommend delayed CT imaging through the area
… may represent thymus vs thoracic aortic injury (in a 2 year old who fell down stairs)
Some trauma professionals will read the radiology report and then immediately order more xrays. Others will critically look at the report, the patient’s clinical status and mechanism of injury, and then decide they are not necessary. I am firmly in the latter camp.
But why do some just follow the rad’s suggestions? I believe there are two major camps:
Those that are afraid of being sued if they don’t do everything suggested, because they’ve done everything and shouldn’t miss the diagnosis
Those that don’t completely understand what is known about trauma mechanisms and injury and think the radiologist does
Bottom line: The radiologist is your consultant. While they are good at reading images, they do not know the nuances of trauma. Plus, they didn’t get to see the patient so they don’t have the full context for their read. First, talk to the rad so they know what happened to the patient and what you are looking for. Then critically look at their read. If the mechanism doesn’t support the diagnosis, or they are requesting unusual or unneeded studies, don’t get them! Just document your rationale clearly in the record. This provides best patient care, and minimizes the potential complications (and radiation exposure) from unnecessary tests.
This 11 minute video provides information on the cervical spine clearance process in awake patients, reviews activity restrictions associated with the use of cervical collars, and discusses information about specific type of collars. It is designed for ED nurses and non-ED nurses who may encounter cervical spine collars.
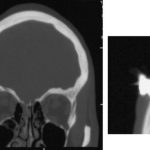
The patient was a 27 year old intoxicated male who was uncooperative with police in France. The offending object is a Taser dart, which was fired at him for control. The dart was not noticed when he was released from custody, and he later presented to hospital with a headache! The dart was removed by a neurosurgeon and he was discharged uneventfully a week later.
Reference: A brain penetration after Taser injury: controversies regarding Taser gun safety. Forensic Science International, ePub 21 April 2012 ahead of print.
Home of the Trauma Professional's Blog
Do you want to get a daily email every time there’s a new post? See what I’m up to.