Algorithm For Operative Management of Blunt Hepatic Trauma
The Western Trauma Association has just published guidelines on decision-making when faced with hepatic injury in the OR. The algorithm is based on the available literature, which contains little prospective, randomized trial data. Nonetheless, it is a valuable tool that can be used to develop your own institution-specific protocol.
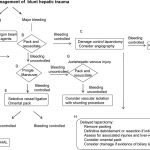
The algorithm is fairly self-explanatory. Click on the image above to read the annotated text for details on each step. Note: this requires full access to the Journal of Trauma.
Some key points in this algorithm:
- Simple hemostatic maneuvers are usually successful with minor bleeding (A).
- Sequential use of more involved maneuvers is indicated for major bleeding. In order, they are packing (B), Pringle maneuver (D), selective vessel ligation within the liver (E), and finally selective hepatic artery ligation (F).
- Damage control laparotomy and interventional radiology are useful adjuncts.
Tomorrow I’ll write about the nonoperative blunt hepatic trauma algorithm. Click here to view it.
Reference: Western Trauma Association/Critical Decisions in Trauma: operative management of adult blunt hepatic trauma. J Trauma 71(1):1-5, 2011.

