Resuscitative endovascular balloon occlusion of the aorta (REBOA) is all the rage. Trauma professionals attending meetings and update courses can count on an update on this interesting technology. But what is it, exactly, and does it work?
REBOA has been around in one form or another for 60 years! In theory, there are five steps for using this technique.
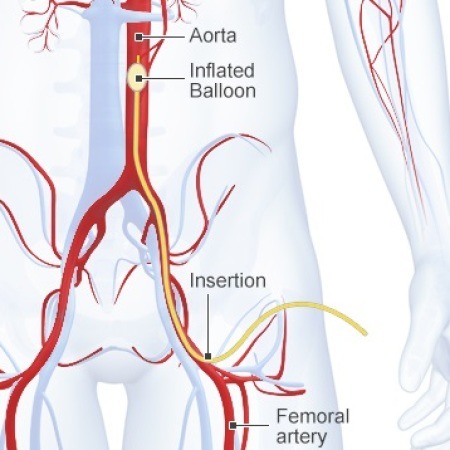
Access a femoral artery using Seldinger technique
Insert a balloon catheter and move it into position proximal to the suspected aortic injury
Inflate the balloon to decrease blood loss at the site of injury
Once the injury has been addressed in the OR, slowly deflate the balloon
Then remove it
It’s basically a way of cross-clamping the aorta within the abdomen noninvasively before the patient is opened in the OR. Here’s a diagram that shows what this looks like. Simple, right?
The authors of a recent paper performed an epidemiologic study analyzing data from the Japan Trauma Data Bank over an 8 year period. They performed some sophisticated analyses to try to reduce the usual issues that occur when perusing typical trauma data bank data.
Here are the factoids:
Over 45,000 patient records were reviewed, and 452 were included in the study. This is a very large number, as relatively few centers use this technique.
The REBOA patients were very badly injured, with a median ISS of 35 and an overall high mortality (76%)
The non-REBOA matched patients were less severely injured, with a median ISS of 13 and a 16% mortality
When matched for probability of survival using TRISS methodology, the REBOA patients had a significantly higher mortality
Bottom line: What does this mean? Basically, that there is an association with higher mortality given similar injury severity and physiologic compromise, in Japan. The study is another piece in the jigsaw puzzle, and not a good one. Sure, things may be done differently in other countries. And the use of REBOA as a “last ditch effort” certainly may result in higher mortality. But it may not be all it’s cracked up to be. Any use of this technique should be critically evaluated, preferably as part of a well designed study. It’s not for the unprepared or faint of heart.
Reference: Survival of severe blunt trauma patients treated with resuscitative endovascular balloon occlusion of the aorta compared with propensity score-adjusted untreated patients. J Trauma 78(4):721-728, 2015.
Home of the Trauma Professional's Blog
Do you want to get a daily email every time there’s a new post? See what I’m up to.