Finally, the chest is open and the tamponade has been relieved. But your patient has little volume. In order to conserve any circulating blood and pump it only to the heart and the head, it’s time to cross clamp the aorta. This task is best left to the surgeon, because it is not a simple matter.
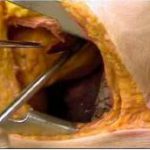
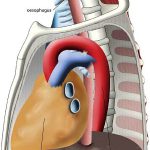
First, you have to locate the aorta, ideally somewhere just above the diaphragm. Unfortunately, if the patient is hypovolemic it’s very difficult to distinguish the aorta from the esophagus, which lie right next to each other (see picture above). In order to make them feel different, insert a gastric tube through the mouth or nose.
Next, separate the aorta and esophagus. They are both covered by pleura. The structure nearest you without the tube in it will be the aorta. Sometimes it’s possible to use a finger to dissect through the pleura and around the aorta. However, the younger the patient, the tougher this tissue is. It may be necessary to incise the pleura with scissors while your assistant holds the lung anteriorly, our of the way.
Finally, once you can pass a finger completely around the aorta, use it to guide the placement of a gently curved DeBakey type clamp (see picture on the left). Squeeze it until it clicks once, and you are done! Now rapidly infuse warmed blood into the patient and run to the OR!
Related posts: