Ugh! What have we come to? And don’t get me
started regarding the electronic medical record. It is true, the burden of documenting what we do in
order to get paid continues to increase. And, of course, this takes time.
And we don’t get paid for the time we spend doing this documentation.
The next
logical step? Hire cheap labor to do the documentation! This is becoming a
fairly common practice, unfortunately. The next abstract is from MetroHealth in
Cleveland. They looked at the impact of hiring scribes from both time and money
standpoints. Two five-month periods were reviewed, with and then without
scribes. Hold on, the numbers here will make your head spin!
Here are the factoids:
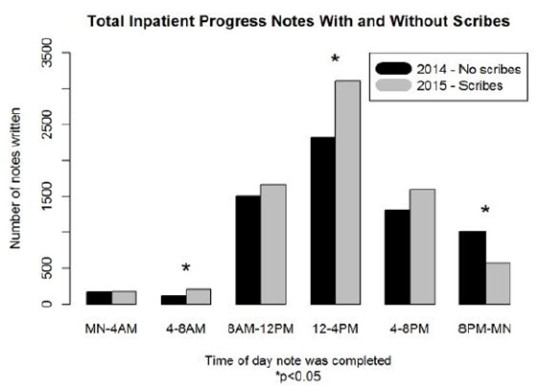
- A total of 9726 notes were written in the no-scribe period, and 10933
were written with scribes - Despite the fact that there were 407 fewer patient-days during the
scribe period, 882 more inpatient notes were written - More progress notes were written early in the day with scribes, and
fewer were written during the evening hours - The number of notes written after patient discharge decreased from
12.7% to 8.4% when using scribes - Charge capture increased by $32 per patient-day (?!)
- The additional scribe notes resulted in an extra
$316K in charges generated
Bottom
line: It’s just so annoying to think that we actually have to stoop to
something like this. The scribes cost this program about $33K. They generated
$316K. The paper estimates that they were actually paid about 20% of this, or
$63,000. So each of the eight trauma surgeons in this program collected an
extra $8,000 over the 5-month period.
So, is it
worth it? Maybe. The extra charges collected seem insignificant. But, if the
surgeon is actually able to dedicate less time to documenting, and this allows
them to spend more time operating (which is what really pays the bills), then
perhaps it is. I’m not easily convinced, though.
Reference:
Trauma surgeons save lives – scribes save trauma surgeons! EAST 2016 Poster
abstract #16.