The Eastern Association for the Surgery of Trauma (EAST) has been helping trauma professionals through the publication of practice guidelines for more than 15 years. Members of EAST donate their time to review reams of literature, good and bad, to try to determine the answers to common or puzzling clinical questions.
Why follow a practice guideline? Quite simply, if properly developed, a guideline represents our best understanding of the “correct” answer to the question posed. And as many of you who follow this blog already know, things that “seem to make sense” frequently are totally wrong. Your own experience is poignant, but the pooled experience of the many others who contributed to research on the topic in question is much more significant.
So on the the practice guideline for blunt traumatic aortic injury (BTAI). This one answers three questions. I will list each, followed by the conclusions reached through the literature review.
1. In patients with suspected BTAI, which diagnostic modality should be chosen: CT angiography of the chest, or conventional catheter angiography?
– Catheter angiography was the standard for decades. When the first EAST guideline on this topic was released 15 years ago, CT angiography was only a level III recommendation because experience with it was lacking. CT technology has advanced rapidly, with multiple detectors, helical scanning, and incredible computing power. Although the quality of the evidence is somewhat low, the panel strongly recommends the use of CT angiography due to its ready availability, speed, low invasiveness, and ability to detect and define other injuries.
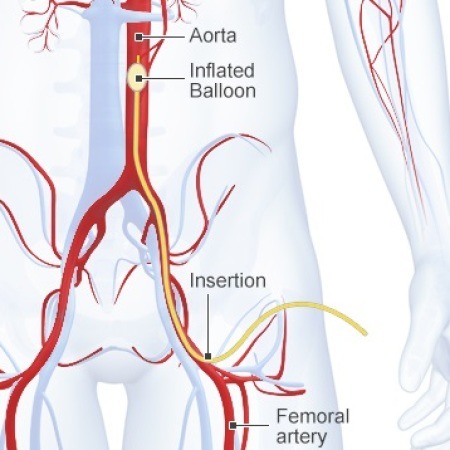
2. Should endovascular or open repair be selected in order to minimize stroke, renal failure, paraplegia, and death?
– Once again, the quality of available data is so so. However, it was possible to detect differences in outcome in comparative studies. The panel strongly recommends the use of endovascular repair in patients who do not have contraindications due to its lower blood loss, mortality, and paraplegia, and equivalent risk of stroke. Furthermore, it is performed more frequently now than open repair, and experience is thus greater at many institutions, further reducing complications.
3. Should the repair be performed immediately or delayed in order to minimize stroke, renal failure, paraplegia, and death?
– Literature review revealed that the incidence of renal failure and paraplegia were lower with delayed repair, while renal failure was the same in patients with significant associated injuries. There was benefit to delaying repair until resuscitation was achieved and any other life threatening injuries were addressed. The panel recommends that delayed repair be carried out once these other conditions have been corrected. The procedure should not be delayed until the next morning for the convenience of the surgeons.
Related posts:
Reference: Evaluation and management of blunt traumatic aortic injury: a practice guideline from the Eastern Association for the Surgery of Trauma. 78(1):136-146, 2015.