The radiologist made me order that (unnecessary) test! I’ve heard this excuse many, many times. Do these phrases look familiar?
… recommend clinical correlation
… correlation with CT may be of value
… recommend delayed CT imaging through the area
… may represent thymus vs thoracic aortic injury (in a 2 year old who fell down stairs)
Some trauma professionals will read the radiology report and then immediately order more xrays. Others will critically look at the report, the patient’s clinical status and mechanism of injury, and then decide they are not necessary. I am firmly in the latter camp.
But why do some just follow the rad’s suggestions? I believe there are two major camps:
Those that are afraid of being sued if they don’t do everything suggested, because they’ve done everything and shouldn’t miss the diagnosis
Those that don’t completely understand what is known about trauma mechanisms and injury and think the radiologist does
Bottom line: The radiologist is your consultant. While they are good at reading images, they do not know the nuances of trauma. Plus, they didn’t get to see the patient so they don’t have the full context for their read. First, talk to the rad so they know what happened to the patient and what you are looking for. Then critically look at their read. If the mechanism doesn’t support the diagnosis, or they are requesting unusual or unneeded studies, don’t get them! Just document your rationale clearly in the record. This provides best patient care, and minimizes the potential complications (and radiation exposure) from unnecessary tests.
This 11 minute video provides information on the cervical spine clearance process in awake patients, reviews activity restrictions associated with the use of cervical collars, and discusses information about specific type of collars. It is designed for ED nurses and non-ED nurses who may encounter cervical spine collars.
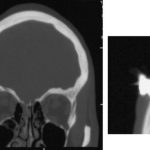
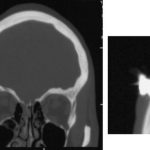
The patient was a 27 year old intoxicated male who was uncooperative with police in France. The offending object is a Taser dart, which was fired at him for control. The dart was not noticed when he was released from custody, and he later presented to hospital with a headache! The dart was removed by a neurosurgeon and he was discharged uneventfully a week later.
Reference: A brain penetration after Taser injury: controversies regarding Taser gun safety. Forensic Science International, ePub 21 April 2012 ahead of print.
This is the third and final topic that I discussed at the 25th Penn Trauma Reunion last Friday. Printer technology has progressed from dot-matrix printers (pushing ink out of a cloth ribbon with little metal pins) to laser printers (fusing dye rolled onto the paper) to inkjet printers (blowing little dots of ink onto paper out of a cartridge).
The next logical step was to go beyond printing with small flat dots of ink and using small spheres of plastic. These tiny spheres can be layered on top of each other using a 3D printer using the the same inkjet type technology and then fused together using a laser. These printers are popular in manufacturing, where they can be used to quickly create prototypes or small parts. Orthopedic surgeons have been using them to print out 3D representations of complex fractures to plan reconstructive surgery (click here for details).
Now consider replacing the little plastic spheres with various cell types cultured from a patient. Load up the “ink” cartridges and start printing some tissue! Anthony Atala runs the Institute for Regenerative Medicine at Wake Forest University and is a pioneer in using this technique. He is able to print 10×10 cm skin grafts on pigs with good results (read about it here). Atala demonstrated the concept of printing whole organs at the TED2011 conference last year. Watch the YouTube video of a kidney being printed here. At this stage of development, it is not a functioning organ, but it’s a great proof of concept.
I believe that this technology is extremely promising. Printing simple human tissues like skin will not be far off. Although it seems farfetched, the picture below shows what is in store in the future. Hopefully, the days of donated organ shortages is coming to an end.