Here’s an interesting clinical case. How would handle this difficult situation?
An 8 year old boy is struck by a car while riding his bicycle. He has obvious head trauma, and medics quickly transport him to your trauma center. He is comatose and posturing with a GCS of 5 (E1 V1 M3). RSI and intubation is carried out, and a full exam is done. Only head trauma is noted, with the right pupil a few millimeters larger than the left. The remainder of the physical exam is unremarkable, with the exception of a few extremity abrasions. FAST is negative, as are portable chest and pelvis xrays.
The child is quickly transported to CT, and this is discovered:
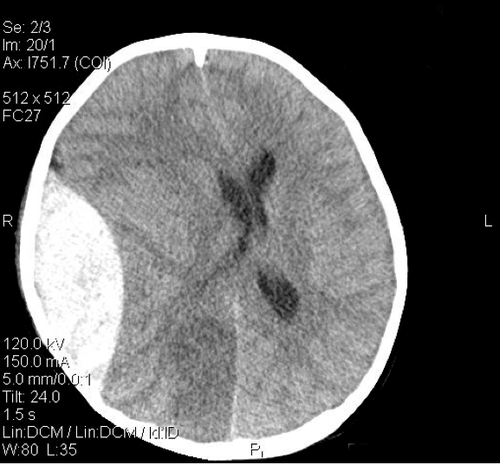
He is immediately transported to the OR, where your pediatric neurosurgeon immediately begins a craniotomy to evacuate the epidural hematoma.
Thirty minutes into the case, you are summoned to the OR because the patient’s blood pressure is dropping and is not responding as expected to fluids and a touch of pressor.
What do you need to think about, and what would you do?
Please comment or tweet all the details. Answers tomorrow!
