Two abstracts that are being presented at the American College of Surgeons Clinical Congress this week use CT scans to predict interesting things. They are things that you would not think a CT scanner should be able to do.
So can we use arcane measurements of things found on CT scan to make accurate predictions about our patients? Sure, if we see very low density bubbles (free air) in the abdomen, it’s pretty likely that some kind of abdominal catastrophe has occurred. Or if their is a large amount of high density fluid (blood) in the left chest after a stab wound, the patient will probably require a chest tube.
But what about other measurements that wouldn’t seem to be related to anything? Could we have found a magic crystal ball here, or is it just wishful thinking?
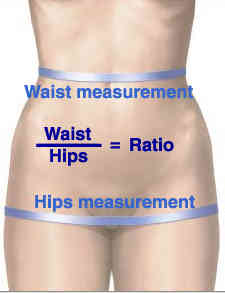
The first abstract evaluated the ability of the waist to hip ratio (WHR) to predict outcomes after trauma. Obviously, this is the width of the waist divided by the width of the body at the hips.
Here are the factoids for this study:
- 555 patients were analyzed retrospectively over 1 year at a Level I trauma center.
- In-hospital complications and death were specifically analyzed
- Using a receiver operating characteristic curve, the authors determined that a magic ratio of 1 was the best predictor
- Complications were significantly higher in the group with WHR>1 (50% vs 19%) as was mortality (17% vs 7%)
- Regression analysis showed that patients with WHR>1 were 4x more likely to have a complication and 3x more likely to die
- WHR was only weakly correlated with BMI
Bottom line: WTF? How can this be, you ask? Just because your patient is a bit “fusiform” in shape, they have a rougher time after trauma? Well, in this case there may actually be some basis for the findings. There are thousands of articles in the literature that have identified that this shape actually is associated with higher complications and mortality in general. And there are already some published trauma papers that have confirmed this association. Interestingly, the BMI was less predictive that the WHR in this study, so this may be a better surrogate measure for obesity.
The number of patients enrolled is reasonable, and the statistics look sound (for just being an abstract). So there may be something here. However, before you start using the “measure tool” on your CT console on every trauma patient, wait for the confirmatory prospective studies to come along.
Tomorrow, a look at a not-so-good study of this type, looking at an even more arcane metric on the CT scan.
Reference: Computed tomorgraphy-measured waist to hip ratio: a reliable predictor of outcomes after trauma. ACS Scientific Forum, trauma abstracts, 2016.