Anatomy is complex and confusing at times. Pretty much everything you can find in the human body has a name. Sometimes it makes sense. Sometimes it’s named after someone famous. And sometimes, it’s just a head-scratcher.
Let’s take the surgical neck of the humerus. Here’s an image of the proximal humerus:
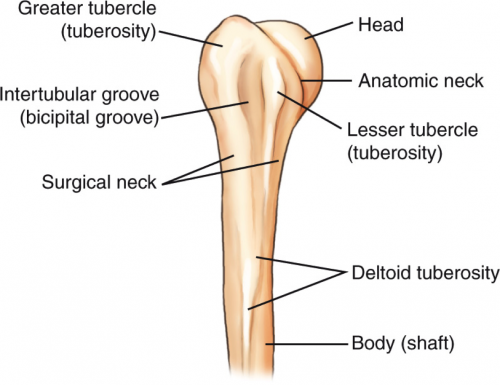
Notice there are two different “necks” of the humerus. You are probably familiar with the anatomic neck from your anatomy classes. But if you are a resident, an orthopedic surgeon, or someone who deals with fractures regularly, you are more familiar with the surgical neck.
The surgical neck of the humerus is the most common fracture site on the proximal humerus. But here’s the kicker. It’s a misnomer!
Just because you see a fracture of the surgical neck of the humerus doesn’t meed it needs surgery! Indeed, many of these fractures are now successfully treated with immobilization in a sling. Your friendly neighborhood orthopedic surgeons will assess fracture stability by looking at the mechanism, exact location, involvement of the tubercles, and motion. Then they will decide on their treatment plan.
Bottom line: Don’t get suckered when someone asks you what operation is usually needed for a fracture of the surgical neck of the humerus!
Related posts: