Several products for compressing the fractured pelvis are available. They range from free and simple (a sheet), to a bit more complicated and expensive. How to decide which product to use? Today, I’ll discuss the four commonly used products. Tomorrow, I’ll look at the science.
First, let’s dispense with the sheet. Yes, it’s very cheap. But it’s not easy to use correctly, and more difficult to secure. Click here to see my post on its use.
There are three commercial products that are commonly used. First is the Pelvic Binder from the company of the same name (www.pelvicbinder.com). It consists of a relatively wide belt with a tensioning mechanism that attaches to the belt using velcro. One size fits all, so you may have to cut down the belt for smaller patients. Proper tension is gauged by being able to insert two fingers under the binder.
Next is the SAM Pelvic Sling from SAM Medical Products (http://www.sammedical.com). This device is a bit fancier, is slimmer, and the inside is more padded. It uses a belt mechanism to tighten and secure the sling. This mechanism automatically limits the amount of force applied to avoid problems with excessive compression. It comes in three sizes, and the standard size fits 98% of the population, they say.
Finally, there is the T-POD from Pyng Medical (http://www.pyng.com/products/t-podresponder). This one looks similar to the Pelvic Binder in terms of width and tensioning. It is also a cut to fit, one size fits all device. It has a pull tab that uses a pulley system to apply tension. Again, two fingers must be inserted to gauge proper tension.
So those are the choices. Tomorrow, I’ll go over some of the data and pricing so you can make intelligent choices about selecting the right device for you.
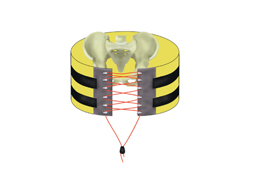
Yesterday, I wrote about the open book, A-P compression mechanism, pelvic fracture. In the “old” days, the recommended management for an unstable pelvis like these was application of an external fixator. In some textbooks, it was even suggested that this should be done (by orthopedics) in the resuscitation room. High volume trauma centers with ortho residents could actually pull this off, but not many others.
As the idea of pelvic orthotic binders caught on (T-POD, sheeting, etc) and was adopted by prehospital providers, and then trauma teams, the use of initial external fixation dropped off. But the idea that external fixation was the most desirable or most effective lingered on. A study from Memphis finally sheds some light on the answer to this question.
A 10 year retrospective review was carried out on patients presenting with multiple or severe pelvic ring fractures who had early stabilization of the pelvis. Stabilization consisted of external fixation early on, and gradually shifted to pelvic orthotic devices over the study period. They ultimately analyzed outcomes for 93 patients in each treatment group.
The authors found that transfusion needs were dramatically reduced with the orthotic devices (5 units vs 17 units at 24 hours) compared to the orthotics. About a quarter of patients in each group went to angiography, and even in those patients the transfusion need remained lower in the orthotic device group. Hospital length of stay was also significantly shorter in this group (17 vs 24 days). There was no difference in mortality.
Bottom line: Although this is a small, retrospective study it easily showed significant results and will probably never be repeated. Use of a pelvic orthotic device (POD) resulted in less blood replacement and shorter stays in hospital. This technique is simple, cheap and quick, an ideal combination. But does a sheet count as an orthotic device? We don’t know. It’s really cheap, but probably a bit less controlled than a POD. If you have a real POD in your ED or your ambulance, use it. If not, apply the sheet, which will be described tomorrow with other binders.
Tomorrow: what’s the “best” pelvic binder?
Reference: Emergent pelvic fixation in patients with exsanguinating pelvic fractures. JACS 204:935-942, 2007.
Pelvic bony injury requires substantial force, and there are several distinct fracture patterns seen. Today, I’ll briefly review the so called A-P force mechanism and its grading.
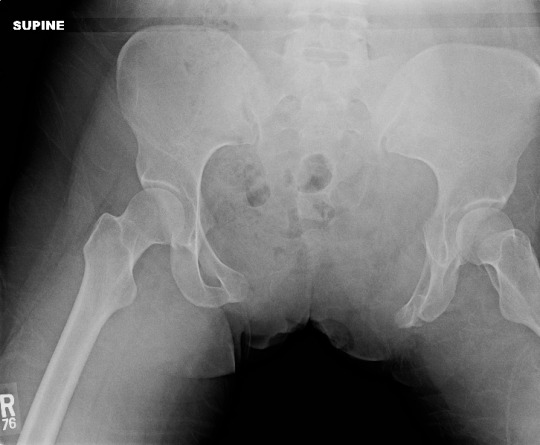
The anterior-posterior (A-P) mechanism frequently results in what many call an “open book” pelvis on x-ray evaluation. It most commonly occurs when something heavy rolls over or crushes the pelvis. We see this in patients who have a vehicle roll over their torso, or are crushed by heavy machinery. The force is applied to the sacrum posteriorly and the anterior portions of the iliac crests. This fulcrum effect displaces one or both iliac wings posteriorly. The flexion point is typically the sacro-iliac joint or the sacral wings. The pubic symphysis pulls apart as the iliac wings move away from their anatomic position.
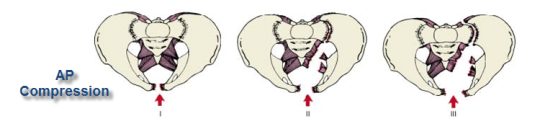
The usual grading system assigns a type subclassification based on the amount of disruption:
Type I – less than 1 inch (2.5cm) of pubic diastasis, or rami are fractured; no significant posterior injury
Type II – more than 1 inch of diastasis; one or both SI joints widened; posterior SI ligament intact; anterior SI, sacrospinous and sacrotuberous ligaments torn
Type III – all anterior and posterior ligaments disrupted
How is this grading system useful? It is generally predictive of hemodynamic instability, resuscitation requirements, and the possibility of concomitant vascular and/or neurologic compromise. However, you can also get a pretty good idea of all of that just looking at the x-ray. But it is helpful in describing the injury to your orthopedic colleagues.
The Eastern Association for the Surgery of Trauma (EAST) has published their most recent set of practice management guidelines. This one addresses prevention of falls in the elderly.
All trauma centers and trauma professionals are seeing more and more elderly patients, and the increase in the number of falls among these individuals is alarming. Most trauma centers are already engaging in some kind of prevention activity. However, their falls prevention efforts are all over the map, and there has been little guidance regarding what works and what does not.
So what can be done? The EAST practice management guideline group performed a methodical sweep of the literature to try to give us some objective information to shape prevention efforts. They addressed six specific questions. I have listed them below, with comments on what the literature shows us about the answers.
Question 1: Should bone mineral-enhancing agents be used? Conditional recommendation. A meta-analysis suggests that giving Vitamin D and calcium supplements tends to decrease fall-related injuries. The optimal dosing was not clear, but cholecalciferol doses of 400-800 IU daily and calcium dosing of 1000 to 1500 mg/day were most commonly used. There was a trend toward improved muscle strength and balance.
Question 2: Should hip protectors be used? Conditional recommendation.
The evidence does show that wearing protectors decreases fall-related injury. However, compliance is usually an issue because they don’t look very cool. See below:
Question 3: Should exercise programs be used? Conditional recommendation. The literature on exercise routines shows a tremendous amount of variability in terms of the specific routines used. However, most studies do demonstrate a reduction in injury with implementation of an exercise program.
Question 4: Should physical environment modifications be made? Conditional recommendation. Conditions in the household are one of the biggest factors for causing falls. Clutter, throw rugs, poorly placed furniture all increase the risk of injury. The literature is extremely variable in the methods or equipment used, so the results are quite variable as well. Overall, home modifications such as grab bar placement, clutter removal, etc. appear to be of benefit.
Question 5: Should risk factor screening be used? Conditionally recommended. Screening for risk factors is not a specific intervention. However, it can and should be used to identify at-risk patients and direct interventions toward specific risk factors (see next question).
Question 6: Should multiple, tailored interventions be used? Strongly recommended.Research shows that if risk factor screening is applied to individuals or larger populations, and interventions directed at the specific factors identified are implemented, very favorable results are possible.
Bottom line: The best results I have personally seen at other trauma centers have been accomplished through risk factor screening and the use of multiple targeted interventions. Many centers address a single factor, or give talks to groups of older, non-injured patients. Although these activities may make us feel good, they probably don’t have the full effect that multifactorial interventions do, as addressed in Question 6.
Elderly falls are a huge problem (and growing). Every trauma center should work on implementing a comprehensive and multi-factorial falls reduction program. And don’t try to reinvent the wheel. Many centers are already doing this, so don’t be shy about borrowing their program components!
Reference:
Prevention of fall-related injuries in the elderly: An Eastern Association for the Surgery of Trauma practice management guideline. J Trauma 81(1):192-206, 2016.
Home of the Trauma Professional's Blog
Do you want to get a daily email every time there’s a new post? See what I’m up to.