Lots of great comments about this case yesterday. So you’re looking for reasons why this 8 year old child is having blood pressure problems while undergoing craniotomy. On first pass through the ABCs, everything looks good. Looks. That’s not enough.
The airway is definitely good. It’s been physically checked. But what about breathing? Lung sounds seem to be good, but in children they can be transmitted from the other side. There are a few solutions. If you have fluoro or quick access to a chest xray, that could be used. However, quickness is the key. If in doubt and the pressure is really becoming a problem, consider empiric needle decompression or finger thoracostomy if you want to avoid chasing with a chest tube on each side.
What about circulation? We’ve ruled out just about every source of bleeding but the abdomen. No FAST? Then why not fall back on DPL? Sure, it’s been a while since you’ve done it. And probably even longer since you’ve done one on a child.
DPL tips for kids: You’re really interested in the tap, not the lavage. If there’s enough bleeding in the abdomen to cause hypotension, you’ll find it quickly. Use open technique (not Seldinger) and insert the catheter far enough to cover all the tiny holes. One reader suggested using a suction cathether (like a Poole sucker). The only issue is one of control so the amount of blood removed can be measured. (Bonus tip: if you ever do the lavage part in a child, use 10cc saline or lactated ringers per kg).
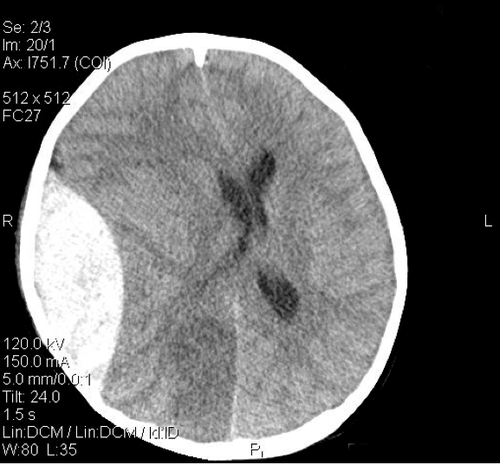
In this case, the chest was negative, and there was no blood in the abdomen. The culprit was D (disability in ATLS jargon). And unfortunately, hypotension from CNS causes is universally an indicator of impending doom.