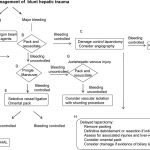
Algorithm For Operative Management of Blunt Hepatic Trauma
The Western Trauma Association has just published guidelines on decision-making when faced with hepatic injury in the OR. The algorithm is based on the available literature, which contains little prospective, randomized trial data. Nonetheless, it is a valuable tool that can be used to develop your own institution-specific protocol.
The algorithm is fairly self-explanatory. Click on the image above to read the annotated text for details on each step. Note: this requires full access to the Journal of Trauma.
Some key points in this algorithm:
Simple hemostatic maneuvers are usually successful with minor bleeding (A).
Sequential use of more involved maneuvers is indicated for major bleeding. In order, they are packing (B), Pringle maneuver (D), selective vessel ligation within the liver (E), and finally selective hepatic artery ligation (F).
Damage control laparotomy and interventional radiology are useful adjuncts.
Tomorrow I’ll write about the nonoperative blunt hepatic trauma algorithm. Click here to view it.
Reference: Western Trauma Association/Critical Decisions in Trauma: operative management of adult blunt hepatic trauma. J Trauma 71(1):1-5, 2011.
The Eastern Association for the Surgery of Trauma is in the process of updating their trauma practice guidelines for liver injury. The first set of guidelines was introduced in 2003, and several advances in management have occurred since. here is a summary of the current status of the guidelines:
Level I recommendations (best quality data):
none
Level II recommendations (good data):
Initial management of hemodynamically stable patients should be nonoperative
CT of the abdomen with IV contrast is the most reliable method to assess severity of liver injury in the hemodynamically stable patient
Unstable patients should undergo operative or endovascular management of their injury, not imaging
Patients with peritonitis should go to the operating room
Age, grade of injury, amount of hemoperitoneum and age are not contraindications to nonoperative management. Only hemodynamic stability matters.
Angiography with embolization should be considered if a contrast blush is seen on CT
Angiography with embolization may also be considered if there is evidence of ongoing blood loss without blush on CT
Nonoperative management should only be considered if continuous monitoring and serial exams can be carried out at your hospital, and if an operating room is immediately available if needed
Level III recommendations (weak data):
Clinical status should dictate need and frequency of followup imaging (my interpretation: only do it if the patient condition changes for the worse)
Interventional modalities may be used to treat complications (ERCP, percutaneous drainage, laparoscopy, etc)
If a patient transiently responds to fluid initially, try angiography with embolization while they are still stable
On Monday, I’ll present the updated guidelines for management of spleen injury.
Reference: Trauma Practice Guideline Update, 24th Annual Scientic Assembly, Eastern Association for the Surgery of Trauma, January 2011.
Home of the Trauma Professional's Blog
Do you want to get a daily email every time there’s a new post? See what I’m up to.