The serial hemoglobin (Hgb) determination. We’ve all done them. Not only trauma professionals, but other in-hospital clinical services as well. But my considered opinion is that they are not of much use. They inflict pain. They wake patients up at inconvenient hours. And they are difficult to interpret. So why do them?
I’m reposting this mini-series on serial hemoglobin draws in light of a new paper that was published in the Journal of Trauma Nursing. It continues next week with Part 2, and then a summary of the new paper.
First, what’s the purpose? Are you looking for trends, or for absolute values? In trauma, the most common reason to order is “to monitor for bleeding from that spleen laceration” or some other organ or fracture complex. But is there some absolute number that should trigger an alarm? If so, what is it? The short answer is, there is no such number. Patients start out at a wide range of baseline values, so it’s impossible to know how much blood they’ve lost using an absolute value. And we don’t use a hemoglobin or hematocrit as a failure criterion for solid organ injury anymore, anyway.
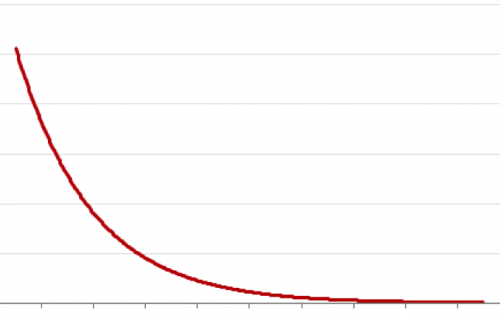
What about trends, then? First, you have to understand the usual equilibration curve of Hgb/Hct after acute blood loss. It’s a hyperbolic curve that reaches equilibrium after about 3 days. So even if your patient bled significantly and stopped immediately, their Hgb will drop for the next 72 hours anyway. If you really want to confuse yourself, give a few liters of crystalloid on top of it all. The equilibration curve will become completely uninterpretable!
And how often should these labs be drawn? Every 6 hours (common)? Every 4 hours (still common)? Every 2 hours (extreme)? Draw them frequently enough, and you can guarantee eventual anemia.
Bottom line: Serial hemoglobin/hematocrit determinations are nearly worthless. They cost a lot of money, they disrupt needed rest, and no one really knows what they mean. For that reason, my center does not even make them a part of our solid organ injury protocol. If bleeding is ongoing and significant, we will finding it by looking at vital signs and good old physical exam first. But if you must, be sure to explicitly state what you will do differently at a certain value or trend line. If you can’t do this and stick to it, then you shouldn’t be ordering these tests in the first place!
In my next post, I’ll discuss a paper that objectively shows the (lack of) utility of this testing method.