A number of scoring systems have been developed to identify FES (Gurd’s and Wilson’s criteria, Schonfeld’s criteria, Lindeque’s criteria to name a few). Unfortunately, none of these are helpful. They were developed in the 1980s as part of the authors’ studies on the use of steroids for treatment, and no one else has taken the time to study their sensitivity and specificity.
Diagnosis of FES is primarily clinical. It relies upon recognition of the principal findings on physical exam, and exclusion of more common conditions that may mimic it.
Here is a template for diagnosing FES:
Is your patient at risk? The vast majority of these patients will have fractures. One, or especially two or more long bone fractures (mostly the femur) are usually present. Other fractures that add risk are those involving the pelvis or bones that contain marrow, such as the ribs and sternum. Patients who have just undergone fracture repair are also at risk and will be discussed in the next section. Finally, patients who have had intraosseous lines placed are also at risk, regardless of the type of infusate.
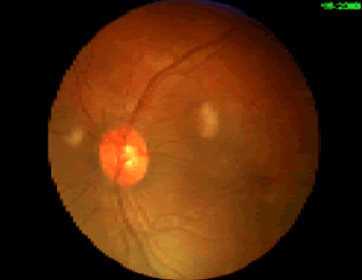
What signs or symptoms have developed? Skin changes are very suggestive of FES if your patient is at risk. However, rashes are common manifestations of contact allergies, drug reactions, infectious diseases, and many other conditions. If those are ruled out, then the presence of risk factors plus a rash is sufficient to make the diagnosis.
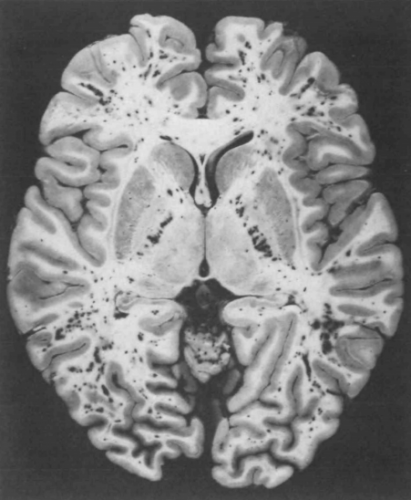
Mental status changes are more difficult to pin on FES, even though it is a more common initial presentation than the rash. Since this is a trauma patient, you must rule out delayed manifestations of head trauma. Urgent CT of the head is required to do so. And typically, there will be no specific findings that point to FES. It is always a diagnosis of exclusion.
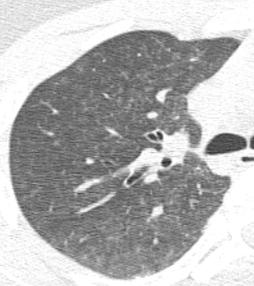
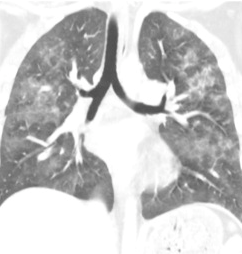
Pulmonary dysfunction requires a search for the usual suspects. A good physical examination of the chest coupled with a chest x-ray will help identify pneumothorax, hemothorax, or pneumonia. A chest CT may be indicated if pulmonary embolism is suspected.
Once other more common clinical problems have been eliminated, you are left with the diagnosis of FES. There are no specific lab tests to draw, and more invasive studies are neither helpful nor indicated. Fat embolism syndrome is a diagnosis of exclusion.
Next, the relationship of fat embolism and orthopedic surgery.