The first modern paper published on REBOA for trauma in 2011 was really a description of the technique using the catheters available “back in the day” (only 5 years ago!). There were six papers published in 2012 through 2015 which I term the years of the pig, as we sought to figure out if this was really something we could and should do in people. The answer in all six was a resounding yes.
Next, a Japanese group published a retrospective database review of 45,153 humans, of whom 452 patients underwent REBOA placement. REBOA has been in use in Japan for a number of years. It is typically placed by emergency physicians, for whom it is a competency requirement for board certification. Raw mortality numbers were worse (76% with REBOA vs 16% without). This poor result persisted even when the patients were matched for their ISS difference (35 with REBOA vs 13 without).
This was troubling, but it was a registry study and questions also arose regarding experience levels of the clinicians. Major trauma is a less frequent event in Japan, and trauma surgeons do not typically take in-house call, which may have resulted in delays to definitive control of hemorrhage.
Another Japanese study published last year was a single center review of 24 insertions over a 7-year period. REBOA survival was 29% vs a TRISS probability of survival rate of only 13%. Better news! However, temper this with one vascular injury and two ischemic limbs, all of which required amputation.
And now, more human studies are beginning to trickle down into the journals, with promising results.
Tomorrow: The real bottom line.
Direct links to the REBOA series:
- REBOA: What is it?
- Who will benefit from it?
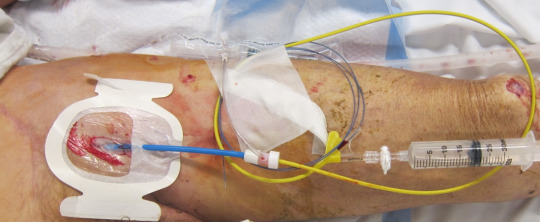
- How do you do it? Part 1
- How do you do it? Part 2
- What are the results?
- The real bottom line
- References