I’m going to be (re)sharing the laws of trauma over the next few posts. I’ve identified a total of eleven over the past 12 years, and I wanted to share them with you.
But first, I’d like to share another trauma surgeon’s observations. Dr. Norman McSwain was an icon in trauma surgery during the early years of my career.
I knew Norm for decades and literally grew up reading about his advancements and accomplishments. Unfortunately, he passed nine years ago. It’s interesting that one never truly appreciates the magnitude of a colleague’s achievements until the person is gone.
Norm was a skilled surgeon and teacher, but his achievements were felt far outside his home in Louisiana. He was an early member of the ACS Committee on Trauma, and was very involved in the development of the Advanced Trauma Life Support and Prehospital Trauma Life Support courses. He is credited with developing the original EMS programs in both Kansas, where he took his first faculty position out of residency, and in New Orleans, his home for the remainder of his life. He spent his career at the Charity Hospital there, weathering multiple political storms over the years, as well as the big one, Hurricane Katrina. He was instrumental in achieving Level I Trauma Center status for its replacement, Interim LSU Hospital.
Norm’s accomplishments are, as many of his contemporaries who have left us, too numerous to count. I certainly won’t try to recount them here. But it was his charm, his love for his charges, and his willingness to teach every trauma professional that will always be remembered.
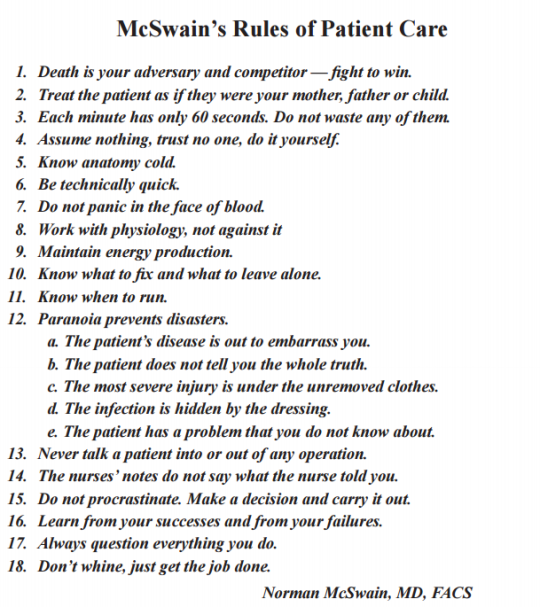
I’ll leave you with his 18 rules of patient care. They are timeless and will serve you well regardless of your degree and level of medical training.
In my next post, I’ll start explaining the eleven laws that I’ve developed.
The VIP syndrome occurs in healthcare when a celebrity or other well-connected “important” person receives a level of care that the average person does not. This situation was first documented in a paper published in the 1960s, which noted that VIP patients have worse outcomes.
Who is a VIP? It may be a celebrity. A family member. Or even a colleague. Or the President of the United States. VIPs (or their healthcare providers) may expect to get special access to care and that the care will be of higher quality than that provided to others. Healthcare providers often grant this extra access through returned phone calls and preferential access to their clinic or office. The provider tries to provide a higher quality of care by ordering additional tests and involving more consultants. This idea ignores the fact that we already provide the best care we know how, and money or fame can’t buy any better.
Unfortunately, trying to provide better care sets up the VIP for a higher complication rate and a greater chance of death. Healthcare consists of several intertwined systems that generally have found their most efficient processes and lowest complication rates. Any disturbance in this equilibrium of tests, consultants, or nursing care moves this equilibrium away from its safety point.
Every test has its own set of possible complications. Each consultant feels compelled to add something to the evaluation, which usually means even more tests and more potential complications. Once too many consultants are involved, there is no “captain of the ship,” and care can become fragmented, even more inefficient, and dangerous.
How do we avoid the VIP Syndrome? First, explain these facts to the VIPs, making sure to impress upon them that requesting or receiving ” different ” care may be dangerous to their health. Explain the same things to all providers who will be involved in their care. Finally, do not stray from how you “normally” do things. Order the same tests you usually would, use the same consultants, and take control of all of their recommendations, trying to do things your usual way. This will provide the VIP with the best care possible, which is actually the same as what everybody else gets.
References:
“The VIP Syndrome”: A Clinical Study in Hospital Psychiatry. Weintraub, Journal of Mental and Nervous Disease, 138(2): 181-193, 1964.
Caring for VIPs: nine principles. Cleve Clin J Med. 2011 Feb;78(2):90-4. doi: 10.3949/ccjm.78a.10113. PMID: 21285340.
As I was browsing through my journal list this week, I ran into an interesting title for an article that is currently in press.
“The use of radio-opaque markers is medical dogma”
Catchy, especially since I love writing about dogma vs what is really supported by the literature. The author questions the justification of this practice and posits that there are risks to extrapolating information based on radiographs with markers placed by the trauma team.
OLYMPUS DIGITAL CAMERA
The author first reviewed the literature on the use of markers for penetrating injury, which started only recently, in 2002. Markers were initially used to precisely locate the penetration site since skin wounds (obviously) don’t show up on X-rays. Typically, these were just plain old paper clips. Some trauma professionals placed them directly over the wound. Others un-bent them and fashioned them into shapes that pointed to the exact location of the wound.
With the growing usage of CT scans to evaluate stable patients, modifications to the marker were made. Small arrow markers designed for use on x-rays were frequently used. However, even the very small ones could cause enough scatter on a CT scan to interfere with diagnosis. At some centers, Vitamin E capsules were taped on top of the wound. But thankfully, there are now special markers that can pinpoint the wound without degrading the tomographic image.
The author goes on to describe how gunshot wounds specifically are difficult to assess with a marker. Although the exact surface location may be noted, the underlying injuries vary due to size, distance, velocity, and trajectory change from tissue density or bone strikes. He also notes that it may not be wise to place a marker into a bloody field in a potentially combative patients.
The article concludes that the use of this technique for identifying anything other than surface location of penetrations lacks clinical evidence and is based only on expert opinion. Which essentially makes it dogma.
Bottom line: Here are my thoughts. First, the use of markers on penetrating wounds has been going on for much longer than the 20 years found in the trauma literature reviewed here. It has been a common practice among trauma surgeons for many, many decades. Most “seasoned” (old) trauma surgeons have been doing and teaching this for their entire careers.
I concur that we have techniques like CT scan available to us now that provide an excellent view of the penetration trajectory. The skin wound is usually apparent on the scan, but may be improved with the use of a CT-approved marker.
So why still do this for the patient arriving in your trauma bay? An experienced trauma surgeon can get a good sense of the trajectory based on the entry point, the exit wound, and the location of any retained bullet or fragments. Rapid placement of some kind of marker on all wounds followed by a quick image allows them to roughly predict what was hit, and assess the possibility that there might be bleeding that would drive the team straight to the operating room. It can help direct the surgical exploration if imaging was unnecessary or contraindicated.
So yes, this is dogma. The reality is that no one will ever be able to design a study that definitively evaluates the very soft outcomes that result from using this technique. But every senior trauma surgeon can easily cite numerous examples in their career when this method has been extremely useful. The lack of a study only means that there will never be any evidence-based guideline for the use of this technique. However, it is still acceptable to have a protocol based on substantial clinical experience. But as with all dogma, once that definitive study finally does comes along, the protocol must be modified to adhere to the findings of the study.
For now, keep using those markers! And I’m very interested in comments from both old and young trauma professionals on this topic.
Reference: The Use of Radio-opaque Markers is Medical Dogma, doi:10.1111/acem.1485, Dec 2023.
Ever been in a trauma activation where it seems like the first thing that happens is that someone steps up to the patient with the ultrasound probe in hand? And then it takes 5 minutes of pushing and prodding to get the exam done?
Well, it’s not supposed to be that way. The whole point of adhering to the usual ATLS protocol is to ensure that the patient stays alive through and well after your exam. And FAST is not part of the primary or secondary surveys, it is an adjunct.
As always, there are a few exceptions to the rule above.
If an unstable patient arrives without an obvious source of bleeding, FAST of the abdomen should be able to detect if a large hemoperitoneum is present. This will expedite the patient’s transfer to the OR.
A patient in cardiac arrest may benefit from a quick FAST to determine if cardiac activity is present. If not, it may be time to terminate resuscitation.
Many people say that FAST and physical exam can and should happen simultaneously.
In principle, I agree. My previous statements were based on the way that we organize our trauma team and trauma activations at this hospital. The reality is that everyone’s team is different and they may run their trauma activations differently.
The goal is to get all information critical to keeping your patient alive as quickly as possible. In some cases, knowing if there is a significant amount of fluid in the abdomen can be very important. Most trauma resuscitation schemes at trauma centers make use of multiple personnel so that various portions of the patient evaluation can be carried out simultaneously.
But there is also a tradeoff between speed, trauma team size and number of trainees. Centers with fewer or no trainees will have a leaner team with experienced examiners and more room around the patient. At our hospital, we have 8 people clustered immediately around the patient, with half of them being surgery or emergency medicine residents. This means it is more difficult for a physician to step in and do a FAST exam easily. So typically, this physician is the same resident doing the torso portion of the physical exam. This is the main reason for my exhortation to wait until the end of the physical exam and do the FAST quickly.
Bottom line: With the exceptions noted above, always complete the ATLS primary and secondary surveys first. Then pull out the ultrasound machine, but be quick about it. If it takes more than about 60 seconds to do the exam, someone probably needs a little more practice.
Some trauma centers receive a significant number of transfers from referring hospitals. Much of the time, a portion of the workup has already been done by the outside hospital. If the patient meets one or more of your trauma activation criteria, do you still need to activate your team when they arrive?
And the answer is: sometimes. But probably not that often.
Think about it. The reason you should be activating your team is that you suspect the patient may have an injury that demands rapid diagnosis and treatment. The purpose of any trauma activation is speed. Rapid evaluation. Fast lab results. Quick access to CT scan or OR. If a significant amount of time has already passed (transported to an outside hospital, worked up for an hour or two, then transported to you), then it is less likely that a trauma activation will benefit the patient.
There are four classes of trauma activation criteria. I’ll touch on each one and the need to activate in a delayed fashion if present, in priority order.
Physiologic. If there is a significant disturbance in vital signs while in transit to you (hypotension, tachycardia, respiratory problems, coma), then you must activate. Something else is going on that needs to be corrected as soon as the patient arrives. And remember the two mandatory ACS criteria that fall into this category: respiratory compromise/need for an emergent airway, and patients receiving blood to maintain vital signs. But a patient who needed an airway who is already intubated and no longer compromised does not need to be a trauma activation.
Anatomic. Most simple anatomic criteria (e.g. long bone or pelvic fractures) do not need a trauma activation unless the patient is beginning to show signs of physiologic compromise. However, anatomic criteria that require rapid treatment or access to the OR (proximal amputations, mangled or pulseless extremities, spinal cord injury) should be activated.
Mechanism. Most of the vague mechanistic criteria (falls, pedestrian struck, vehicle intrusion) do not require trauma activation after transfer to you. But once again, if the mechanism suggests a need for further rapid diagnosis or treatment (penetrating injury to abdomen), then activate.
Comorbidities. This includes underlying diseases, extremes of age, and pregnancy. In general, these will not require trauma activation after they arrive.
Bottom line: In many cases, the patient transferred in from another hospital will not need to be a trauma activation, especially if they have been reasonably assessed there. The patient should be rapidly eyeballed by your emergency physicians, and if there is any doubt about their condition, activate then.
However, if little workup was done at the outside hospital (my preference), and the injuries are “fresh” (less than a few hours old), then definitely call your team.
And finally, if the patient meets any of the ACS hard criteria for activation (this includes hypotension, transfusing blood, and respiratory compromise), don’t hesitate to trigger the activation!
Home of the Trauma Professional's Blog
Do you want to get a daily email every time there’s a new post? See what I’m up to.