Contrast blush is always a concern when seen on CT of the abdomen for trauma. It can represent one of two things, and both are bad:
- Active extravasation of contrast
- Splenic pseudoaneurysm
These two clinical issues can be distinguished by looking at the location of the contrast and its persistence. A pseudoaneurysm is located within the parenchyma, and the contrast will wash away, so it will not be visible on delayed images. Contrast that extends beyond the parenchyma or persists in delayed views represents active bleeding. In either case, the failure rate of nonoperative management exceeds 80% in adults without additional measures being taken.
Clinically, these patients usually act as if they are losing volume and require additional crystalloid and/or blood transfusion. The natural history in adults is for bleeding to continue or for the pseudoaneurysm to rupture, resulting in a quick trip to the operating room.
If vital signs can be maintained with fluids and blood, a trip to interventional radiology may solve the problem. Selective or nonselective embolization can be carried out and patients with only a few bleeding points can be spared operation. However, if multiple bleeding areas are seen, it is probably better to head to the OR for splenorrhaphy or splenectomy.
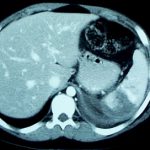
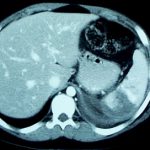
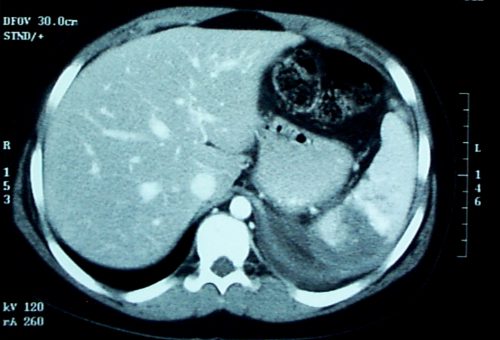
The image below shows likely areas of extravasation. They are a bit large to be pseudoaneurysms.
Children are different than adults. Extravasation from spleen injuries in prepubescent children frequently stops on its own. Angiography should only be used if the child is failing nonoperative management.