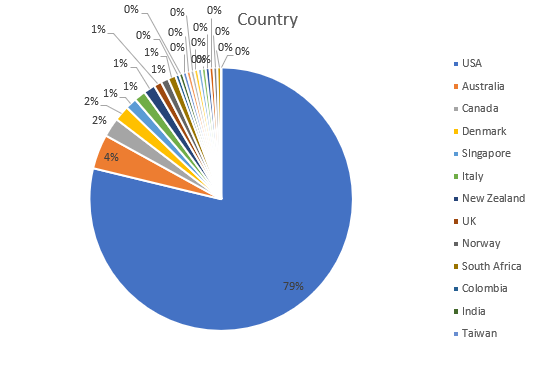
Again, thanks for all who submitted their survey answers. Here’s a rundown of the answers provided by US respondents. A few duplicates from the same hospitals have been merged into single answers for them. Total number of US centers for the tables below is 149.
Level of trauma center
| Level I | 83 |
| Level II | 37 |
| Level III | 15 |
| Level IV | 1 |
| Level V | 2 |
| Seeking verification/designation | 1 |
| No level | 10 |
How many ED thoracotomies are performed per year at your hospital?
| A few per year (<6) | 83 |
| About every month (6-15) | 35 |
| A couple of times a month (16-30) | 23 |
| About every week (31-52) | 8 |
What type of trauma do you perform ED thoracotomy for?
| Both blunt and penetrating | 79 |
| Penetrating | 64 |
| Blunt | 5 |
Do you use a practice guideline for ED thoracotomy?
| Yes | 86 |
| No | 47 |
| I’m not sure | 15 |
Do you use REBOA in your ED?
| No | 88 |
| Yes | 58 |
| I’m not sure | 3 |
And now for the questions you’ve been waiting for!
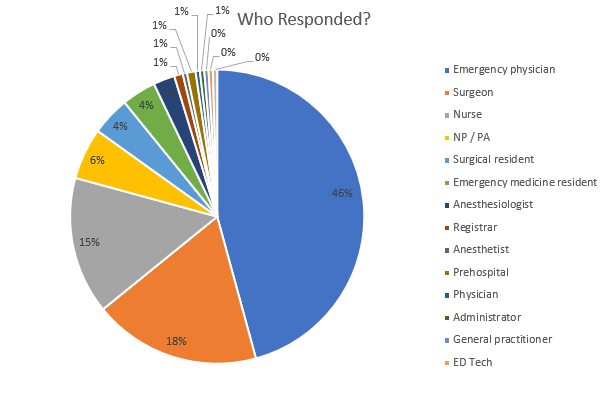
Who could perform ED thoracotomy at your hospital? (n=149)
| Surgeon | 145 | |
| Emergency physician | 109 | |
| Surgical resident / fellow | 93 | |
| Emergency medicine resident | 66 | |
| APP (PA, NP) | 2 | at one Level I and one Level V |
| Family physician | 1 | at one Level V |
| Family medicine resident | 1 | at one Level V |
Who usually performs ED thoracotomy at your hospital? (n=149)
| Surgeon | 115 | |
| Emergency physician | 25 | |
| Surgical resident / fellow | 69 | |
| Emergency medicine resident | 17 | |
| Never done one | 3 | |
| Family physician or family nurse practitioner | 1 | at one Level V |
Who usually performs ED thoracotomy at your hospital? (By trauma center level)
| Level | I (n=83) | II (n=37) | III (n=15) |
| Surgeon | 64 | 35 | 11 |
| Emergency physician | 8 | 3 | 6 |
| Surgical resident | 63 | 4 | 1 |
| Emergency medicine resident | 12 | 1 | 2 |
| No one | 0 | 0 | 1 |
Join me tomorrow when I review the international data!