In my last post, I reviewed the three screening systems for blunt carotid and vertebral artery injury (BCVI). Today, we’ll look at grading them.
Just ten years ago, it was a major production to identify BCVI. Then, CT angiography was still in its early days, and scanner resolution and radiologist experience were significant issues that impacted accuracy.
We’ve come a long way in a relatively short period of time, and current-day scanners now have more than adequate resolution. It’s also more common to have a radiologist with special skills reading these studies, the neuroradiologist. For these reasons, CT angiography has become the standard for diagnosis. It is also the most cost-effective. Only in sporadic cases do we need to obtain a conventional contrast angiogram.
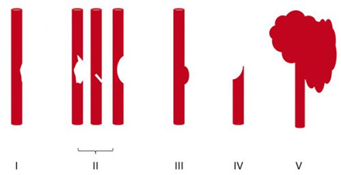
Once the study has been obtained, it’s time to identify and classify the injury. The Denver group is also responsible for bringing us the grading system for BCVI. See the diagram below.
Here are the details:
Grade I: A mild intimal irregularity is seen. Note the abnormally narrowed area, representing a minor intimal injury, possibly with a small amount of clot.
Grade II: This grade has several presentations. There may be an intraluminal thrombosis/hematoma with (left) or without (right) an intimal flap, or a flap alone (center).
Grade III: There is a full-thickness injury to the vessel with a contained extraluminal extravasation (pseudoaneurysm)
Grade IV: The vessel is completely occluded by a flap or thrombus
Grade V: The artery is transected and freely extravasating
Here’s a nice diagram:
Remember, we always grade things for a reason! Ultimately, the injury grade will translate into the selection of treatment. We’ll cover that in my next post.
Reference: Blunt carotid arterial injuries: implications of a new grading scale. J Trauma. 1999;47(5): 845-53.
