Initial CT scan evaluation for blunt trauma patients is fairly standardized. The usual palate consists of scans of the head, cervical spine, chest, abdomen and pelvis. Some choose their “colors” individually, and others just slop everything on the canvas.
However, there are a few other scans that are occasionally helpful and/or necessary. Think soft tissue views, or CT angiogram of the neck, or CT angiogram of potential extremity vascular injuries.
Another study that is occasionally needed but many times unnecessarily ordered is the dedicated CT of the facial bones. This study spans the entire area from mandible to frontal sinus and is performed using finer cuts to display greater detail.

The unfortunate truth is that a large number of dedicated facial CTs either do not show fractures, or show fractures that don’t require operation. The scan does deliver a nice dose of radiation, though. Is there any way to be more selective about ordering it?
About 10 years ago, a plastic surgery group in Madison developed what came to be called the “Wisconsin criteria” for ordering facial imaging. Here they are:
- Bony step-off
- Periorbital ecchymosis
- GCS < 14
- Malocclusion
- Missing teeth
The authors claimed 97% sensitivity and 2.6% missed fracture rate, although external validation suggested those numbers were a bit generous. The Plastic Surgery group from the University of Minnesota and Regions Hospital recently re-studied these criteria with a large number of patients, looking at accuracy as well as cost-savings.
They performed a retrospective review of 1000 patients (based on a power analysis) who had a facial CT and adequate documentation of the Wisconsin criteria in the chart. Here are the factoids in table form: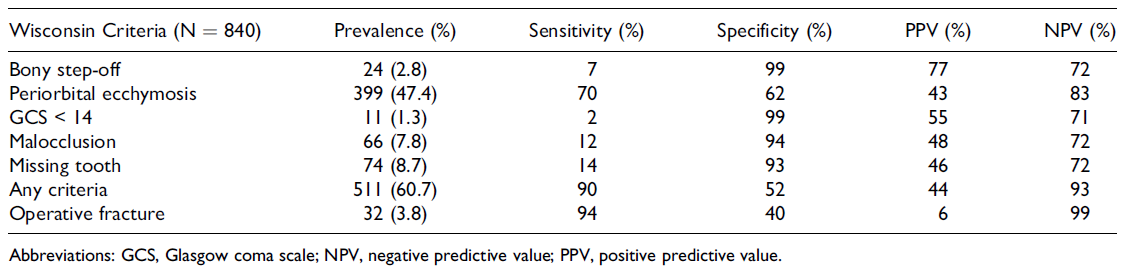
(click table for larger copy)
- Periorbital ecchymosis was the most common criterion, which had the highest sensitivity of 70% (terrible)
- The other criteria fared even worse from a sensitivity standpoint
- But if you roll them all up together, the presence of any one of the five yielded a 90% sensitivity (true positives) and 52% specificity (true negatives)
- The negative predictive value was 93% if none of the criteria were present, which means it’s a good tool for ruling out the need for a CT scan
- The overall missed fracture rate was 2.8%, and only 0.12% for ones that required operation
- Cost savings by limiting CT to patients who met the criteria was over $300K in 2014
Bottom line: What to do? It’s clear that using the absence of any of the Wisconsin criteria to avoid a facial CT scan is helpful. This makes sense, because 4 of the 5 criteria are findings on facial exam. But it also means that a lot of scans will still get done for low sensitivity criteria.
How about this? Since nearly all of these patients will have head and cervical CT scans, review the head scan first for facial fractures. Single, non-displaced fractures are nearly always nonoperative in nature. If patterns of fractures are present, or there are significant displacements, a dedicated facial scan will be very helpful in determining operative management.
But remember, the head CT does not include the mandible. A good physical exam and occlusion check is mandatory, and any suspicion of injury should prompt a full scan of the face.
Thanks to Chris Stewart, the lead author on this study for sending it to me for review.
Rreference: Validation of the “Wisconsin criteria” for obtaining dedicated facial imaging and its financial impact at a Level I trauma center. Craniomaxillofacial Trauma & Recon 13(1):4-8, 2020.
