My last post provided some history about the original Glasgow Coma Scale (GCS). Today, I’ll provide some of the finer details of measuring the components of the current iteration of GCS (not GCS-40). I will list out the individual scale values, and explain some of the most misunderstood.
As you know, there are three components to the GCS. Let’s examine each:
Eye Opening
- 4 – This is an easy one. The eyes are open, and they are opened spontaneously.
- 3 – Eyes open to your voice. If your patient is asleep and they awaken, the E score is actually 4. If they only open their eyes to repeated voice prompts, then it is a 3.
- 2 – Eyes open only to pain or stimulation. This is typically tested by squeezing a fingernail, but the exam should progress as described in the Nuances section below.
- 1 – This one is easy, too. The eyes don’t open, no matter what.
What if the eyes are swollen shut? Then record it as E1c (c = closed).
Verbal Response
- 5 – Your patient is oriented and converses with you spontaneously.
- 4 – Confused. This means that you can talk with your patient and they respond in sentences, but you can detect some confusion or disorientation based on their speech.
- 3 – Inappropriate words. Remember it this way: your patient speaks like a 3-year-old. They can say a few words but can’t construct a meaningful sentence.
- 2 – Incomprehensible sounds. This means that your patient may moan or make noises, but does not form any words.
- 1 – No verbal response at all.
If the airway is controlled with an endotracheal tube, then the score is recorded as V1t.
Motor response
- 6 – Your patient obeys commands.
- 5 – Localizes to pain. Your patient will move toward a painful stimulus in an attempt to remove it. They can move their arms/hands above their chin in response to facial stimulation.
- 4 – Withdrawal from pain. Patients cannot move their arms above the chin.
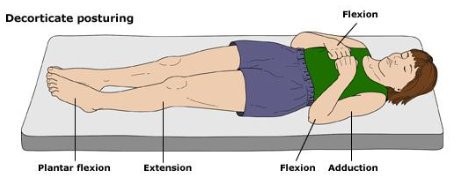
- 3 – Flexor response (decorticate posturing). This score, and the next one (2), are the ones that I always confuse. Just remember that the patients reach for the “core.” They flex their forearm and wrist, clench their fist, extend their legs, and point their toes (plantar flex).
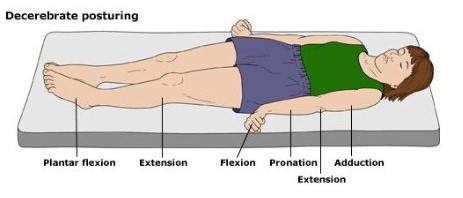
- 2 – Extensor response (decerebrate posturing). These patients bring their arms to their sides (adduct), extend the elbow but flex the wrist and fingers, and pronate the forearms. Legs and feet are the same as above.
- 1 – No response to stimuli.
Nuances
- Record the entire score. This means all components and modifiers. An example would be E3 V4 M4 = 11, or E1c V1t M3 = 5, or E1 V1 M2rt M3lt = 4/5
- Alcohol or drug intoxication will interfere with accurate measurement of the GCS, especially with the verbal and eye-opening components.
- If the motor score is asymmetric (higher on one side than the other), record the higher score. Or better yet, break out the motor scores for both sides so your friendly, neighborhood neurosurgeon has a better idea of what is going on.
- Stimulation should proceed from fingernail squeeze, to pinching the trapezius muscle, to pressure in the supra-orbital notch, in that order. The sternal rub is to be discouraged, as it can lead to bruising.
In my next post, I’ll describe the differences in the Pediatric Glasgow Coma Scale.
